CLINUVEL Communiqué III
Dear shareholders, friends,
INTRODUCTION
During the lockdowns our team has had plenty of time to review our existentiae ratio; why is it that we address our thematics day in day out? Across the Group, we became immobile but yet connected by the cable of empathy we all feel for our patient populations, and furthering our work is the main motivator. For our Singaporean teams, the prospect of taking new products to markets, is shared as a unique and rare objective in a relatively young country. In EPP, we have found a population who have been housebound all their lives – call it a permanent lockdown. We all now realise the precise meaning of forced isolation. Part of our choosing new indications for melanocortins encapsulates the factor of clinical affinity.
In this News Communiqué III, we are reviewing some of the activities of CLINUVEL over the past 2 months. As per tradition, we provide commentary to macro events and deliberations as to how these may influence overall business.
The upswing in viral numbers in March and April has notably been a concern as parts of Europe went into third lock-down. Italy, Germany, France, Netherlands, and parts of Spain were affected, while the UK had announced long term measures to curtail the R-number (see earlier News Communiqués in 2020). While the state of Victoria in Australia is currently in third lock-down, we see the relaxation of measures in other parts of the world as indicative of growing confidence in the vaccination programs.
During recent News Communiqués, we shared our views on the probability of inflation and in particular, its impact on our sector. Since March, we are now facing real inflation and the question is how this rise in prices has emerged so swiftly. Expressed as Consumer Price Index (CPI), in February the US recorded 1.7% and in March 2.6% real increase in prices compared to the same period in 2020. On an annual basis, the Brookings Institute predicts an annualised increase of prices of 4.1%. I find myself asking the rhetorical question as discussed during the recent AGM of Berkshire Hathaway, openly posing ‘why do we all accept rising prices at these times’. Equally in our sector, we see a disproportionate price increase in services, raw materials, and essential goods and supplies.
We think back at Yellen, the FED’s Chairman under Obama, who set a target 2% inflation rate. While she has been a formidable force in monetary policy, one lesson to keep in mind is that many economists have been proven wrong when it comes to the depth of the current crisis, the rate of recovery, predictions of the markets and the swift rise in prices. While the US economy is growing, as well as the Eurozone’s, the developed countries have benefited from the central injection of liquidity in the markets with the latest US$1.9 trillion stimulus package pushed through by the Biden Administration. It is one of the factors for a faster than anticipated rise in prices. However, consumer prices have risen disproportionately high, a trend which is also seen in healthcare and pharmaceuticals. Against the backdrop of rising pharmaceutical drug prices, we expand on CLINUVEL’s position later in this Communiqué. Our suppliers have put through as much as a 20% increase, on supplies and services and this swell requires caution and foresight in financial management, whereby we continuously assess value for money and alternatives.
Overall, we foresee an upward adjustment of interest rates later this year or in 2022. The FED and central banks will be forced to intervene at this rate of recovery and economic expansion. The current reheating of our depressed economies is not a new phenomenon, the economic programs of Roosevelt and Obama both aimed at reinvigorating employment against the backdrop of inflation. The liquidity provided to society is already leading to a surge in new jobs and positions in Europe and US. While there is resistance from Powell and FOMC to touch interest rates, his UK counterpart Bailey has made public remarks that cutting below 0% would no longer stimulate the UK Economy; we await the Bank of England’s decision as to whether rates can stay at 0.1% on 24 June.
Some key lessons from COVID are drawn as it impacts CLINUVEL. First the dependence and reactionary rethink of supply chains, the interconnected sector and reliance on key suppliers required our attention. Second, the revision of our processes to accommodate ‘working from home’ as a lasting phenomenon. We foresee that some of our offices will continue part-time working from home coupled with a regimen of two to three days in the office. This trend alone shifts our thinking about the necessity of expenditures towards central offices within business districts. Third, the future expansion of the Company to optimise innovation and distribution. As our economies become more automated and less reliant on human workforce, I also anticipate the introduction of AI and more expenses towards IT-led solutions and services. In life sciences, the rise of e-devices, self-reported outcomes through wearable technologies and medical solutions, may well apply to our particular business.
Amid all these changes, one is called for a calm demeanor to oversee the secular trends in the markets. We all realise that independence and value is secured by preservation of cash sufficient to withstand market swings when money becomes dear and equities start to correct, while shareholders benefit from consistency.
One outstanding consequence of the pandemic is a greater appreciation for healthcare from administrations and the business community, whereby more focus is given to supply chains, prevention, and manufacturing.
Moreover, the realisation that dependence on other surrounding nations in terms of health crises superimposes an additional risk on societies, we see how many nations are trying to provide for future health crises by establishing their own manufacturing facilities. CLINUVEL’s expansion in manufacturing befits this global trend and as we progress our plans, we will follow periodically with news on this topic.
Centricity in Clinical and Personal Care
In our modern approach to patient care and personal care, we introduced a model which appears to deviate from the norm in pharmaceuticals and yet has worked well for us. Following the approach in many service industries and customer-focused enterprises, our emphasis and commitment is to remain in contact with the end-user on a long-term basis. The six-figure investments to establish systems and processes stems from CLINUVEL’s approach to follow up and assist patients where needed. The entire company is operating under a virtual service agreement with our patients and medical community. Our universal care goes beyond the industrial mode. Our operations are geared towards actively finding healthcare providers, insurers, physical assistance, transport, and ensuring longitudinal safety reporting. All these facilities encompass what I see as the 21st century relationship with the medical end-user, the patient and general beneficiaries of our healthcare products.
This precarious approach to directly communicate with patients is bound by strict rules (General Data Protection Regulation) and follows internal training of selected professionals who monitor the adequate use of personal data through a databank, exclusively to be used for purposes related to the clinical assistance required. The repository of data is subject to external audits whereby other members of the Company do not gain access to ensure patients’ confidentiality.
Under the European Regulation (EU) 2016/679 on the protection of personal data, there are clear boundaries of what a company is allowed to do with regard to patients’ personal data. In addition, in respecting the Charter of Fundamental Rights of the European Union, one has to observe the right of protection of personal data as a fundamental right in its Article 8. It means that everyone has the right to protection of data concerning individuals and that processing must be fair, for specified purposes and on the basis of the consent of the person concerned. Another important part is that it gives people the right to access data concerning themselves and have incorrect information rectified. The latter does not apply when answering to their request to assist in insurance matters.
Many North-American organisations have had to make changes to comply with the GDPR, and also our US operations have had to adapt to the EU regulations, such as asking for explicit consent and revising user terms of agreement. In general, one can state that the same set of data protection rules apply across the EU.
Shifting this theme to the entry of US data in CLINUVEL’s Global EPP Disease Registry (GEDR), the transfer of cross-border data requires robust systems and oversight to manage the process of storage and analyses. The ultimate goal of these systems is for our teams together with EU and US regulators, to be able surveil the safety of SCENESSE® in the long term. We are at a position whereby both systems are functioning well and well accepted by EMA and FDA. From an investment point of view, it has been worthwhile for the company to manage these systems itself contrary to the usual outsourcing of these services.
Recent discussions with US institutional investors revolved around CLINUVEL’s approach to its clinical program, the role of patients and patient organisations. Although in these discussions we cannot disclose more information than what is in the public domain, we share here a general summary on CLINUVEL’s main strategy on centricity of diseases states:
- Emphasis on patients but also their immediate families
- Decisions taken based on feedback from patient communities and
- Genuine demand for treatment/product without solicitation or intervention of the Company, whereby we prioritise patients who have:
- been “forgotten, neglected”, untreated (unmet clinical needs);
- lack of alternative treatment (lack of comparable); and
- show similarity in disease states and behaviour cross-border (uniformity).
The question is whether each pharmaceutical company is acting towards these objectives, and our analysts and institutional investors drew first conclusions that CUV as an organisation distinguishes itself from others in its centricity.
General Operations
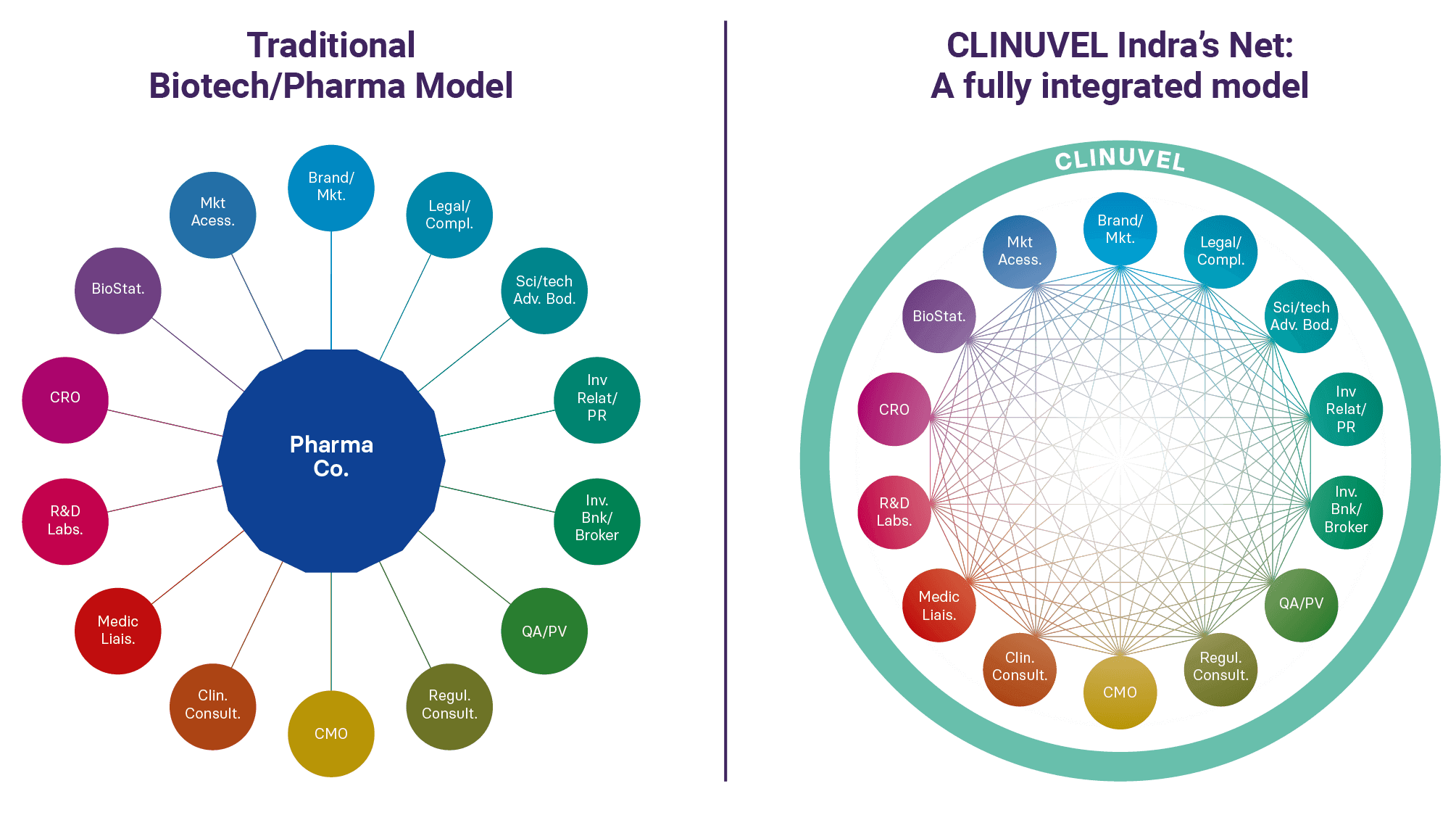
I see the CUV business model best explained in terms of Indra’s net, a Buddhist concept where interconnectedness plays a big part of the construct. Most decisions taken by our managers are interdependent and are seldom a direction or position taken in isolation. As part of this view of interdependence, all our managers are therefore cross-functional and involved in more than their core specialty or background; with that comes integration from the day they join the group. And to introduce the obvious paradox, at the same time we ask there to be a degree of disconnection from possible cognitive biases, to arrive at sound and sometimes unpopular decisions. In the evaluation of the Company, we wish to see our teams communicate not only the outcomes and data, but – within the boundaries of disclosure ability – also why our managers take certain directional choices.
As a further quick note to our four divisions, statistically most corporate mergers fail to integrate the acquired company. Therefore, our current mode to continue building from within is a safer remedy to render the group competitive.
On 12 April, we released our Strategic Update II to which the feedback on content and format has been positive. Here, we had chosen to answer some of the questions relating to corporate choices and strategy. Whereas traditionally, pharma and biotech companies provide news as it occurs, our Communications, Branding and Marketing (CBM) team initiated a new format of providing shareholder updates by not only focusing on progress, but also on explanations and criteria chosen to grow and expand the Company. We will continue this series in Strategic Update III, planned for October.
On 29 April, we released the Group’s quarterly financials (ending 31 March). As iterated, due to the gyrations in receipts one cannot provide a real-time snapshot on supply of our lead product, but it does provide a general idea of commercial operations. We continue to provide these quarterly statements as a courtesy to our long-term shareholders.
As to the financial management of the Company, we received specific questions how CUV intends to manage the Company if a downturn in the markets eventually unfolds. One cannot claim to predict the direction markets will take; however, we do frequently adjust our variable costs taking into account cyclical corrections evoked by unexpected events, whereby each macro event is often characterised as ‘unexpected’.
While financial decisions are frequently and routinely made among Board and Executive Management, we can openly speak to the issue of leverage. Highly geared companies in markets of low conjuncture tend to be more vulnerable, there is nothing new here. However, actors in high-risk industries tend to underestimate the compounded effect of market corrections, as the institutional reactions often lead to retreat from equities. With small to mid-cap companies the first to experience the on-market redemptions, one needs to realise that current success does not make one insusceptible to these cataclysms. The cumulative spiral of financial distress in pharmaceuticals often originates from debt burden, service levels and need to enter refinance deals when conditions have unexpectedly turned against the issuer. Hence, experience through various economic cycles has driven the need to steer CLINUVEL away from the fringes or zones of financial peril, and the influence we can have over debt, cost effectiveness and rate of investments. Eventually, we are called to manage a company with the view to achieve longevity and sustainability. Those who recognise and fit this approach will gravitate towards the Company.
Global Drug Pricing
The supply of essential “COVID” drugs such as ketamine, prednisone, vasopressin, and oxytocin has attracted much press in Europe and US. With the imminent demand and shortage of drugs, it was inevitable that drug prices would increase. Mainstream press has commented on pharmaceutical companies taking advantage of the COVID pandemic by implementing drug price hikes. It is regrettable and somewhat deplorable that journalists, analysts, and commentators are unable to separate in their headlines the wheat from the chaff.
Without retreating into a full defence mode, naturally we do a 360-degree view on our own behaviour concerning drug pricing, implemented openly since 2017. Following on from that introspection, I believe we will need to give more prominence to the fact that CUV is NOT being commented on as a company that stands out in its drug pricing. For NOT having increased its price of afamelanotide since 2017, NOT having corrected for CPI and (as stated in News Communiqué II) NOT having been commented on for having absorbed currency fluctuations and general price increases from its suppliers of more than 20% over the past 5 years. We are operating very differently from the pack. Some of our analysts comment that CLINUVEL – in managing market access – has outperformed the majority of its peers.
Gauging from global data obtained from Fiercepharma, GoodRx and the Health Care Cost Institute, one can glean more depth on the price increases in the pharmaceutical industry versus CLINUVEL’s consistent price policy being adhered to. Last January, a review of the drugs taught that 601 price increases were recorded at an average of 5.8% compared to 2020.
Staying with the US, the “Most Favored Nation” initiative, first proposed by democratic candidate Bernie Sanders in 2017 (News Communiqués 2017-2018), and used later by the Trump Administration, was recently scrutinised by a federal judge, who derailed the plan. We will watch the next few months how the Biden Administration will manage pharmaceutical pricing strategies.
In Europe, reform of drug prices is a subject of discussion in many countries, whereby attention is given to Advanced Therapy Medicinal Products (ATMPs). As part of its business, CLINUVEL is in continuous dialogue with EU payors and insurers, however – in all its objectivity – there can’t be any component in our strategy to scrutinise the approach and transparency on price setting in the European context concerning SCENESSE®.
This consistent and uniform approach to market access equally reflects our policies, mode of operation and importantly, our pledge to let physicians and patients reach consensus on the demand of our innovative product. We have expressed before that we believe it is not for a pharmaceutical company to send sales representatives and sales personnel to doctors’ offices to boost its sales. In line with this view, CLINUVEL does not possess sales teams or distribution agents – just to highlight our differing approach to pharmaceutical supply in general. In our model, a pharmaceutical drug’s demand is solely dictated by the end-user, without assigning a role for the Company other than to supply on clinical demand.
In the discussions with private insurers, national payors, intermediaries, advisory bodies, and state insurers, we characteristically disclose in each country the number of adult patients and children eligible for treatment and calculate a realistic penetration of the population ahead of annual supply. These precise calculations are the result of 10 to 15 years of investment, intrinsic knowhow of our teams and shared with the respective payors in each country.
This consistent and uniform approach to market access equally reflects our policies, mode of operation and importantly our pledge to let physicians and patients reach consensus on the demand of our innovative product.
We have worked since 2010 on the basis that Real World Evidence (RWE) – meaning clinical data demonstrating evidence that prescribers and patients want to provide and continue receiving treatment – would form the basis for our development of SCENESSE® in EPP. We had the foresight that economic conditions would change in the future, and insurers would want proof of how a drug is used or prescribed under real time conditions – this phenomenon is now accepted in the European Union as real-world evidence.
In evaluating the systemic photoprotective therapy introduced to the market following five years of distribution, it is most satisfying to see that our teams have not made a single error in projecting “the eligible and treatable number of patients per annum” neither in the European Economic Area or United States. In plain terms, the past 15 years our team’s gathered knowledge and market intelligence on the number of patients and number of implants to be supplied per country, but also per province or state: I believe this clinico-commercial attitude is the least one could expect from a pharmaceutical company. Precise knowledge on budget impacts per country, per province.
With this pledge CLINUVEL has never exceeded any annual budget of insurers allocated to the drug or maximum projection of SCENESSE®, but always underbid the maximum threshold. Following a clear and unwavering commercial strategy, I wish CLINUVEL to be best in class, and this establishes a position of confidence between insurers and Company being built over time. Vice versa, in the unlikely event that our team would be exceeding these annual thresholds per nation, it would naturally allow payors to impose penalties and claw back provisions.
I am quite pleased that we have a team to rely on, and under the guidance of Mr Keamy, Mr Hay and Mrs Colucci, the pledge to national payors has been exemplary. In this play, it can only be expected that payors and advisory bodies keep their end of the bargain too, year on year. In time, we will keep informing you on the pricing landscape the EU and US.
In contrast to the pressures exerted by payors Europe-wide, the UK will engage with the public on an expected rise to £500 million per annum for the Innovative Medicines Fund. The situation in Italy is equally promising as the country now has two €500 million funds specifically targeting innovative medicinal products; one covering cancer medicines and one covering treatments for other (rare) diseases. These funds are available for 36 months of treatment, after which regional budgets are assigned.
France is taking a slightly different view via the HAS’s 2020 “Action plan to assess innovative drugs”. As part of this plan, the Committee calls for RWE providing proof of tolerance or efficacy under conditions of real time prescription. The HAS recommends as of 2021 that pharmaceutical companies work with national authorities to systematically collect and analyse real world data.
In Germany, there is equally now an emphasis on real world data and patient registries. Ahead of these developments, in 2014, CLINUVEL set up the European EPP Disease Registry which is meticulously maintained at our cost. Our measures and the rate of prescription determined by physicians and patients should be sufficient to provide clinical and commercial comfort for payors showing that CUV is abiding by all modern rules. Obligatory new discussions with GBA are being held every five years on the real-world experience of EPP patients on SCENESSE® treatment, whereby our teams remain entirely transparent about the ‘objectivated’ clinical benefit patients and physicians express.
Background Information on Research & Development
(Dr Dennis Wright, Chief Scientific Officer)
MELANOCORTINS AND TOPICAL PRODUCTS
CLINUVEL established a global expertise and focus on the medicinal use of specific proopiomelanocortins, hormones, and has commanded scientific authority in the domain of systemic photoprotection. After decades of innovative research and clinical focus, CLINUVEL is currently the only company to have developed and distributed a full body photoprotective therapy for patients affected by the polychromatic – multiple wavelengths – effects of light, as many of you know, treating patients suffering from Erythropoietic Protoporphyria (EPP). Our meaningful and pioneering work is progressing as we make our hormones available to treat the genetic disorder Xeroderma Pigmentosum (XP), patients who are 10,000-fold more susceptible to skin cancer(s) and succumb to these as they are absolute intolerant to UVA and UVB rays.
Our groundbreaking work needed to be translated not only to non-prescriptive, more-easily accessible product lines, but foremost to populations who are not yet addressed in our society.
We presented at an earlier stage, that our Healthcare Solutions team is preparing to launch four product lines, which target specific populations who have not yet been or poorly communicated with. With the CBM team just established, we will actively address these communities.
Naturally, our pioneering work, knowhow and expertise needed to be translated not only to non prescriptive more easily accessible product lines but foremost to populations who are not yet addressed in our society.
Clinical Update
(Dr Dennis Wright, Chief Scientific Officer,
Dr Pilar Bilbao, Head Clinical Operations)
VITILIGO
The FDA organised the first FDA “Virtual Public Meeting on Patient-Focused Drug Development for Vitiligo” on 08 March 2021. For the Division of Dental and Dermatology Products, this is a meaningful step forward as it shows a new focus for an ill-defined disease. On the day, discussions were held on meaningful patient reported outcomes, clinical objectives and importantly the diseases expressed in darker skin populations.
| FDA REGISTERED PARTICIPANTS | |
|---|---|
| Patients |
650 |
| Patients’ representatives |
150 |
| Industry representatives |
200 |
| Healthcare professionals |
50 |
| Academic researchers |
30 |
| Press |
5 |
| Government |
20 |
| Other |
50 |
| Total |
1155 |
On the day, some polling questions were posed to the patients whereby we share the most important ones:
| FDA Question 1: Have you had any of the following treatments or interventions? | |
|---|---|
| Topical steroids |
38% |
| Oral medications |
8% |
| Light therapy |
31% |
| Surgery |
2% |
| Topical depigmentation |
4% |
| Other |
8% |
| None/never |
9% |
Here the contradiction is that although the FDA does not formally recognise narrow band UVB (light therapy) as a standard of care and has not approved NB-UVB as repigmentation therapy in vitiligo, it is the best practice of care. The world’s experts use narrow band UVB as the first resort to stimulate melanocytes, the pigmentation cells of the skin in vitiligo.
| FDA Question 2: Besides medical products or intervention mentioned previously, what else are you doing to manage your vitiligo? | |
|---|---|
| Temporary cosmetic procedures |
25% |
| Dietary supplements |
19% |
| Diet modification |
15% |
| OTC products |
7% |
| Complementary therapies |
6% |
| Counselling/psychological |
8% |
| Other |
2% |
| Not doing any |
18% |
| FDA Question 3: For medical products or interventions, you use, what do you consider to be the most burdensome impacts? | |
|---|---|
| Administration procedure |
10% |
| Therapy provides minimal benefit |
18% |
| Therapy only effective short term |
16% |
| Bothersome side effects of the treatment |
8% |
| Concern about serious risks of treatment |
11% |
| Uncertainty about long-term effects of treatment |
15% |
| Difficult in accessing treatment (insurance/referral) |
16% |
| Other negative impacts |
3% |
| Change in pigmented skin |
4% |
| FDA Question 4: Hypothetically, imagine new topical cream indicated approved by FDA, once a day. It would provide up to 50% repigmentation. Side effects would be: redness, irritation, mild acne and burning? Other side effects: fever, increase of heart rate. Would you use this treatment? | |
|---|---|
| Yes |
36% |
| No |
24% |
| Maybe |
40% |
The head of the FDA’s Division concluded by stating that “there is no denying that vitiligo can result in a loss of one’s identity. It impacts the way others interact with the individual. In some cases, people are unable to get employment, they are voided, and bullied”.
Particularly difficult to hear was that some individuals experience difficulty having their disease taken seriously by physicians who view it as a cosmetic condition and are reluctant to treat it. That is because the physicians believe that patients’ expectation will not be met and will become an exercise ending in frustration.
It was also heard that the current treatment attempts and the impact of treatment make it impossible to do other activities such as work or care for oneself. This is not the kind of treatment burden that anybody wants to live through. Some individuals yearn to have cures and prevention of progression of this disease.
The FDA acknowledged that all patients’ comments were heard on the day. “This forum is important to the FDA, drug companies, researchers and other medical product developers that were in attendance on the day. The Agency hopes that the information provided to the FDA will help advance the science and development of new treatments for patients who would like to have them.”
We refer to our Vitiligo Scientific Communiqués to review our work and scientific progress in generalised vitiligo. The use of afamelanotide in combination with NB-UVB was first published in JAMA Dermatology and later in the Journal of the American Academy of Dermatology. On 29 October 2020 in our Strategic Update I, we provided a summary of vitiligo.
As we speak, our dialogue with the FDA continues to arrive at a preferred design of a clinical trial to finally progress SCENESSE® as a systemic repigmentation therapy in generalised vitiligo. We will report as soon as the agreement with the FDA has been reached.
Arterial Ischaemic Stroke (AIS)
The pandemic has had an impact on the speed of clinical screening of stroke patients in study CUV801. Adjustment and relaxation of inclusion criteria is implemented to ensure patients are enrolled while hospital staff availability is still limited for the conduct of the trial.
In the study CUV801, patients diagnosed with AIS and occlusion distally of M2 branch of the middle cerebral artery, are being included. As a proof of concept, the objective is to assess whether afamelanotide intervention provides a benefit to the arterial supply of the brain.
Particular emphasis is given to the core infarct, that is the irreversibly damaged part of the brain, and the reversible damaged area of the brain, the penumbra, that is brain depleted of blood and oxygen and at risk of tissue death.
The assessment of therapeutic intervention is based on neuroimaging as Computed Tomography Perfusion and Magnetic Resonance Imaging of the brain. The images are analysed and compared between those taken at day of admission of the patient with those obtained after drug treatment.
Afamelanotide is systemically administered at various intervals, while eligible patients are not receiving any other therapy for AIS. Follow up is protocolised during hospital stay and during rehabilitation.
The safety of the stroke patients is the most critical parameter and based on the safety profile of afamelanotide as a selective non-steroidogenic (not acting on the adrenal gland) melanocortin, the study had been approved by the clinical decision makers and Ethics Committee. The preparation has taken years for this trial to be organised and conducted.
… the conduct of CUV801 follows a meticulously planned program whereby the attention given to the aspect of human safety, assessed locoregionally and systemically, has ultimately made this progress possible …
The conduct of CUV801 follows a meticulously planned program whereby the attention given to the aspect of human safety, assessed locoregionally and systemically, has ultimately made this progress possible. Safety of the drug treatment in AIS patients dominates all CLINUVEL’s activities and falls within the established processes of pharmacovigilance. For the CUV team, the CUV801 trial had only emerged since it had established its pharmacovigilance and quality systems within the organisation. A program conducted with the assistance of external safety monitors would have been more demanding and borne additional risk. The current structure allows for direct engagement and collaboration with key clinicians in stroke management.
This AIS trial will be the first human trial, during which a systemic melanocortin is being administered in an acute life-threatening condition.
DNA Repair in Xeroderma Pigmentosum
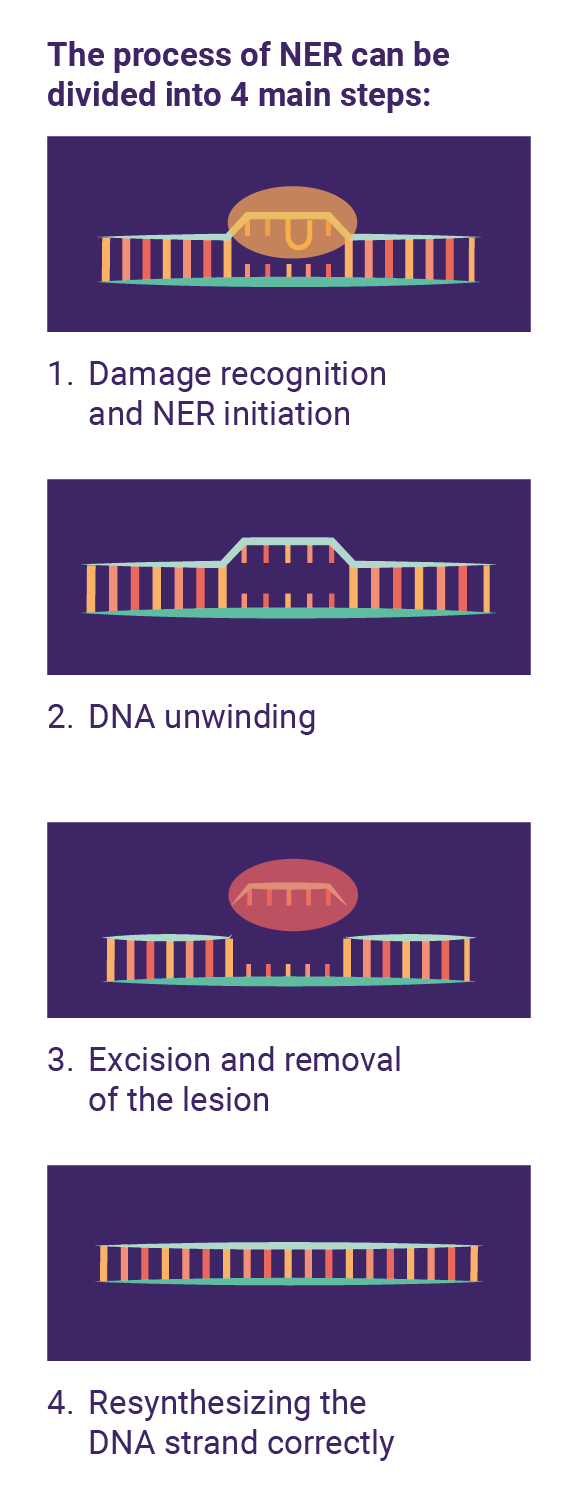
As a reminder, we provide a brief of our fundamental and clinical work on DNA repair to damaged skin. In the most prominent pathway of DNA repair following UV exposure, one distinguishes four phases of Nucleotide Excision Repair (NER). In 2020, we already expanded on these pathways during our News Communiqués and Scientific Communiqués. In a set of sequences, UV damage needs to be recognised by human cells, the damaged strand requires unwinding, removal (excision) and resynthesis of the piece of DNA completed by incision of the damaged fragment.
We also communicated that a regulatory condition to treat XP patients would be to share a set of compelling scientific data from the use of SCENESSE® (afamelanotide 16mg) to make the following arguments to decisions makers, regulatory bodies and ethics committees, institutional review boards:
- clinical safety mid and long-term
- second set of clean toxicology data
- plausibility of clinical success in XP
- systemic photoprotection in the UV and high energy visible (HEV) light spectrum
CUV150 – CUV151- CUV152
Exceptionally, we obtained approvals to proceed our clinical work in XP patients, a first worldwide. Recently, we added the first set of clinical data from the first XP-C patient treated in Europe. The results of the skin biopsies of the first patient are now being processed and available for the authorities. CLINUVEL is only allowed to comment and share these results upon peer review publication of these data.
Our clinical team has collaborated with the expert physicians to design three trials (CUV150, 151 and 152) whereby regulatory authorities, Ethics Committees and patients, consented to skin biopsies taken in XP patients to assess the UV damage.
In addition, XP patients will be subject to narrow band UV radiation delivered on the buttocks to allow for assessment of minimal erythemal exposure (MED), indicating the point of first redness, burn and skin damage.
To our knowledge this is the first time that this type of pharmaceutical trial to evaluate both photoprotection and DNA repair has been approved and organised in XP. The human skin biopsies will give us direct information through
- immunohistochemistry (colouring of skin cells), and
- through cell cultures (patients’ skin cells)
The overall objectives in developing afamelanotide in XP-C and XP-V patients have been summarised as the evaluation of the:
- safety in XP-C patients
- effects on the integrity of their skin (pre-existing poikiloderma)
- effects on photoproducts (following UV exposure)
- effects on nucleotide excision repair (NER) and
- clinical effects as a systemic photoprotective drug
The next stage of XP clinical trials has been finalised in clinical protocols, ethics and regulatory clearance. We expect the first trial to start in weeks to come, as has been communicated by the centres and from the consent provided by patients.
Importantly, we can share that in administering afamelanotide the clinical and analytical objectives in XP and DNA repair will be multifold:
- cellular oxidative damage before and after UV radiation
- formation of photoproducts
- expression of DNA reparative proteins
- systemic photoprotection
Oxidative damage from UV rays follows the formation of radical oxygen species. The ROS mediated oxidation of guanine to 8-oxo-7,8-dihydroguanine (8-oxoG) changes DNA bases which mimic the characteristics of a thymine nucleotide. Since UV damage then often leads to adenine to thymine transition within the newly synthesized DNA strand, mutational risk and skin cancer looms. It is known that up to 2,000 8- oxoG mutations form in mammalian DNA within a normal 24h period, with this figure further increasing after excessive UVR and HEV light exposure.
One of the objectives in our DNA Repair Program and clinical trials is to assess the oxidative damage before and after administration of afamelanotide.
Therefore, one of the objectives in our DNA-Repair Program and its clinical trials, is to assess the oxidative damage before and after administration of afamelanotide. The drug will be dosed at variable intervals for a maximum four months.
Additionally, in these trials we focus on photoproducts, or cyclobutane pyrimidine dimers. The adducts form as a result of abnormal covalent bonds between carbons five and six of adjacent thymine or cytosine nucleotide bases (DNA). In contrast, a non-cyclic bond created between carbon six and four of neighbouring pyrimidines nucleotides generate 6-4PPs. Regardless of these disparities, the presence of an intra-strand cross-linking bond between dipyrimidine sites results in a large bulky distortion of the DNA’s structure.
Finally, we assess in these trials the degree of systemic photoprotection we provide to XP-C and XP-V patients following irradiation of a predetermined skin area(s). We assess the first sign of burns in a group prone to actinic damage and the development of skin cancers.
We regard this clinical concept of ‘assisting DNA repair in XP patients’ as one of the most exciting stage of CLINUVEL’s history, anticipating that melanocortins ultimately will improve the lives of XP-C and XP-V patients.
In discussion, CLINUVEL’s clinical team is presenting its starting point that the ‘cancer development model’ is most apparent in XP patients, since the sequence of catastrophic health events is undisputed:
The trials CUV150, CUV151 and CUV152 are the culmination of 16 years of work preparing to gain t he privilege to treat these unattended patients.

In making afamelanotide available as a marketed systemic photoprotective drug in XP, we anticipate that we will intervene in step 1, 2 and 3 with the aim to decrease the fatal resultant in step 7.
The trials CUV150, CUV151 and CUV152 are the culmination of 16 years of work preparing to gain the privilege to treat these unattended patients.
US Update
(Dr Linda Teng, Director North American Operations)
US Specialty Centers
Over 40 US EPP Specialty Centers have now been trained and accredited and the US team continues to identify and evaluate EPP Specialty Centers located in proximity to EPP patients. Additional EPP Centers have been trained and accredited in the past months. In general, the US team has succeeded – ahead of its targets – to engage all selected physicians and centers across the US where patient clusters have been found. The latest center in Hawaii, demonstrates that we go through each individual state to find a suitably qualified and skillful physicians to treat their patients. The selection process takes much time, but eventually gives our team confidence that the prescriber is motivated and knowledgeable about the disease and treatment.
As written before, our US team are in close communication with the healthcare providers in the EPP Centers so that errors in administration are reduced to minimum or zero. In communicating closely for long periods of time, they get to know staff and prescribers well. Most prescribers are not used to companies following up with their patients for any extended period of time, and the feedback on our teams has been excellent!
As the demand of the product grows, our task is to refer EPP patients to the EPP Centers, provide administrative support on insurance Prior Authorization (PA) and PA renewals. Also, our team gives updates via phone, email, and US clinical newsletters on a quarterly basis. This requires high energy and dedication from the US-AU team, but it works well. In many ways the distribution of other melanocortin products and flaws have taught the US team how to optimise the distribution of the afamelanotide implant.
Most prescribers are not used to companies following up their patients for any extended period of time, and the feedback on our teams has been excellent!
US Patients
To ensure controlled distribution, all EPP patients must obtain a unique patient ID through the www.scenesse.com prior to receiving SCENESSE® treatment. The registration provides data that are protocolised, stored and only used with patients’ consent – exclusively for insurance purposes. Somewhat surprising, throughout the quarter there has been a steady increase on the number of new patients signing up to obtain unique patient IDs, through the Savings Program or Treatment Access. It seems that it has taken some time for many US patients to gain confidence in our system and we have seen a great number of patients taking the time to register.
In addition, new patients have been proactive in scheduling first consultation visits with their nearest center of care to gather information to initiate submissions for Prior Authorizations. Here, daily coordination between patients, physicians and insurers is needed. Currently, US EPP patients are routinely receiving treatments according to the SCENESSE® prescribing information treatment schedule. Strictly limited to those who qualify to prescribe the novel medicine, training and accreditation occurs for each center and medical staff participating in the distribution of SCENESSE®.
Serving as background, the SCENESSE® US Savings Program was launched in 2019. The program provides assistance to eligible EPP patients on their out-of-pocket costs to support patients who need financial assistance and to ensure health equity. The US Savings Program will continue to provide assistance to eligible EPP patients receiving treatment in 2021.
Important is that our US team has received a number of positive comments from EPP patients expressing their appreciation and deep gratitude, and also commenting on the EPP Centers and their professionalism, care, and interest in treating the community of EPP patients. After fighting to get treatment to this particular patient for four months, this came back to Dr Teng’s team which I wanted to share with you:
“The doctors worked together during the injection. Both doctors were so kind, understanding and excited for me to get this injection.
Also, a shout-out to the supporting staff, including the medical student in the room for all the kindness and compassion.
I would give the whole experience a 5 out of 5 rating and would not hesitate to recommend these doctors.
Thank you for all of the wonderful care!”
➢ This really motivates us all, makes us work long hours and I want to thank you for reaching out.
As I reported two months ago, Category I CPT® code for the administration of SCENESSE® is under review by the CPT® Editorial Panel. By obtaining a listed CPT® code for the SCENESSE® administration, the final code is going to expedite much administrative burden and/or eliminate PA approval for the CPT® procedural code, simplify medical billing and facilitate reimbursement for the EPP Centers. We get positive commentary from physicians who seem to appreciate that we make their life easier by having applied for a new Category I CPT® code. The outcome of the review by the CPT® Editorial Panel will be published later this year. The updated CPT® procedural codes become effective for use on January 1, 2022.
With the Category I CPT® code being decided, our US team would have completed a rare journey in the US regarding the introduction of the product to insurers.
To recap, the International Statistical Classification of Diseases and Related Health Problems (ICD-10) is a medical classification list by the World Health Organization (WHO). The ICD-10 is applicable to the treatment provided with SCENESSE® for the specific metabolic disease – Erythropoietic Protoporphyria (EPP) – and deemed a medical necessity. This code is also essential in the billing process by US insurers. Erythropoietic Protoporphyria is listed.
The Healthcare Common Procedure Coding System (HCPCS) allows for the drug coding to be used by healthcare providers for uniform diagnoses, services and care to be characterised. J-codes are part of the billing system used by healthcare providers in order to fulfill billing requirements, and these codes are applicable to injectable prescriptive drugs which are not self-administered. For SCENESSE®, the first J-code as J-7352 has been allocated.
We obtained the National Drug Code (NDC), a unique 10-digit product identifier for human drugs in the United States. The three segments of the NDC identify the labeler, the product, and the commercial package size. The labeler code is assigned by the FDA, while the product and package codes are assigned by CLINUVEL.
With the four codes described above, the US registration journey would have come to an end, our US colleagues executing a strategy and persisting at each challenge.
Of equal importance, in the last weeks, the final part of our US national distribution has come to completion – now fully coordinated by CLINUVEL and centralised in Florida, thereby eliminating many of the logistics and significantly reducing the processing and shipment delivery time by over 50%.
Keeping in mind that the product is transported under specific conditions, under ‘cold-transport’, this reduction of shipment time is significant. It now allows us shorter planning times and clinical allocation times. Clearly, this significantly saves money and time in the long run. More importantly, this shortened timeframe – from order to delivery of the medication – allows US prescribing centers to schedule patients for treatments much more efficiently.
As time goes by, I see how efficiency and operations are becoming increasingly streamlined. Whilst we had originally anticipated a 2-3 year time frame to optimise distribution throughout the US, we now believe that supply and rapid turn-around from insurers can be optimised in 2021, assuming there are no delays due to logistical challenges.
Investor and Public Relations
Malcolm Bull, Head of Investor Relations
Company News Flow
Since our last News Communiqué on 01 April, the Group has continued to progress commercial operations in Europe and the USA and maintained focus on the expansion of research and development activities. Key developments included:
- The DNA Repair Program which commenced in September 2020 was expanded, with the agreement of clinical and academic experts and Ethics Committees, to include patients with Xeroderma Pigmentosum variant (XP-V).
- Chairman Willem Blijdorp announced that CLINUVEL would establish a Manufacturing Division. This fourth division of the Group will focus on manufacturing of novel formulations and products for CLINUVEL and offer research, development and production capacity to other companies and research groups within the biopharmaceutical sector.
- Strategic Update II provided an overview of the new divisional structure of CLINUVEL and status of the expanded clinical program.
- Independent research on CLINUVEL expanded with the initiation of a report by Australian based Wilsons Advisory and Stockbroking Ltd, refer below for more detail.
- The generation of positive cash flow from commercial operations continued in the third quarter of the 2021 financial year, refer below for more details.
CLINUVEL’s announcements are available on the CLINUVEL website and CLINUVEL News. More specifically, Company announcements to the Australian Securities Exchange are available on the investor pages of the CLINUVEL website.
Analyst Coverage of CLINUVEL Expands, Historical Context
Less than three years ago, only one company – Bioshares Australia – issued independent research coverage on CLINUVEL. As CLINUVEL posted positive annual performances from commercial operations, investor interest in the Company increased with a consequent increase in demand for CUV shares. In September 2018, CUV was included in the S&P / ASX 300 Index. In April 2019, Moelis Securities Australia initiated independent research coverage of CLINUVEL. In June 2019, CUV was included in the S&P / ASX 200 Index reflecting further growth in market capitalisation and subsequently, in 2020, other research firms initiated coverage of CLINUVEL – Intelligent Investor, Lonsec Research and Jefferies Australia.
On 26 April 2021, Wilsons became the latest independent research firm to initiate analyst coverage of CUV. Wilsons has over 150 years of experience in the Australian financial sector with a largely institutional and high net worth client base. They followed-up their initiation report on 05 May with a summary of companies focused on a treatment for vitiligo and made positive comment on the opportunity for CLINUVEL’s treatment. Lead Analyst, Dr Shane Storey has monitored CLINUVEL for many years. A salient detail communicated to us was that Dr Storey and his team had spent considerable time reviewing CLINUVEL during 2019 as part of their diligence for another institutional client. However, since the expansion of the Company only took effect after the approval of SCENESSE® by the US Food and Drug Administration on 08 October 2019, Dr Storey and his team were to deepen and update their research during 2020.
Today, there are six independent research firms with an Australian Financial Services License covering CLINUVEL. Independent research coverage of CLINUVEL is welcome as it provides a separate flow of information on and insights into the Company to assist investors to make informed decisions.
| Firm | Date of Latest Coverage | Analysts |
|---|---|---|
| Bioshares | No. 882, 08 March 2021 | David Blake, Mark Pachacz |
| Intelligent Investor | 25 February 2021 | Graham Witcomb |
| Jefferies Australia | 26 February 2021 | David Stanton |
| Lonsec Research | 21 April 2021 | Chad Troja |
| Moelis Australia | 05 March 2021 | Sarah Mann |
| Wilsons Advisory and Stockbroking | 26 April 2021 | Shane Storey, Melissa Benson |
As part of our governance policy, note that CLINUVEL does not edit or redact analyst reports and provides no financial guidance to analysts. Views expressed in the reports may not reflect the status or direction of the Company. The Company does not endorse, confirm, or express a view as to the accuracy of the analyst reports and their forecasts and do not make any representation that its earnings will fall in the range of the analysts’ forecasts. CLINUVEL does not induce, incentivise, or remunerate analysts to publish and recommended CLINUVEL as an investment. We also do not distribute the research reports of analysts since it is directly managed by the institutions and research firms to service their clients. However, we provide below a summary of the independent analysts that cover CUV. More details on the research firms and the analysts can be found on the CLINUVEL website.
In general, the analyst coverage indicates wider and increasing interest in the Company since it is in a growth phase whereby its mandate is to reinvest its funds into diseased and general populations where an unmet need is identified. To date, the majority of the interest – as reflected in CLINUVEL’s register – originates from Europe, United States, Asia, and a minority from Australia. As CLINUVEL is serving markets in the European Economic Area and United States, we understand the origin of the investor interest.
Financial Results – Quarter Ended 31 March 2021
As a recap of our financial position, the generation of positive cash flow from commercial operations continued in the third quarter of 2021. Cash receipts were A$6.524 million and net cash inflow (after operating expenditures) was A$1.986 million in the March quarter 2021. On a financial year to date basis (9 months to March 2021), cash receipts were A$23.805 million, up 26% on the same period of 2020.
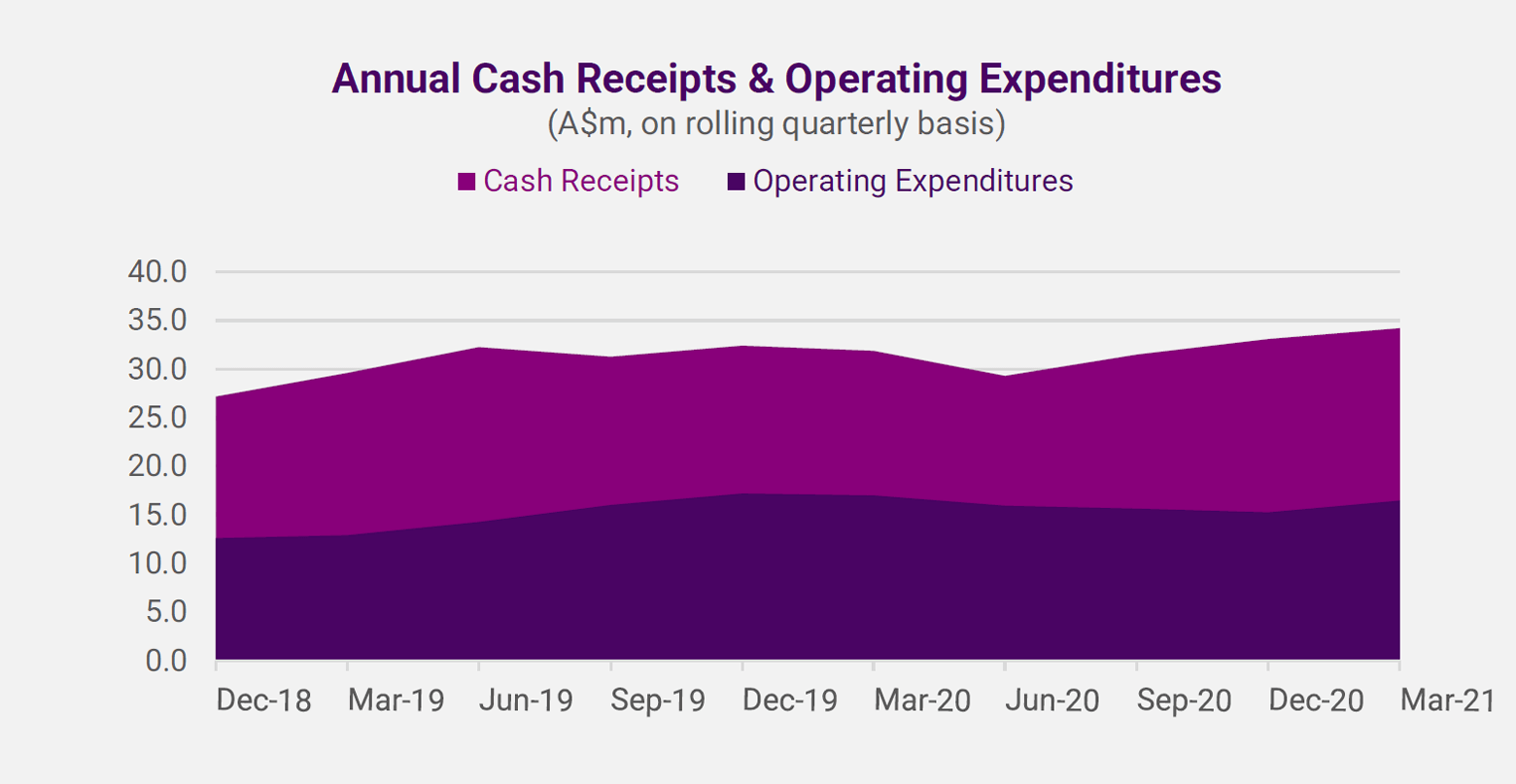
Annual cash receipts in the year ending March 2021 showed a further rise on a quarterly rolling basis (refer graph). The cash results reflect the near normalisation of treatment of SCENESSE® to EPP patients in Europe after an initial adverse Corona virus impact in the June quarter of 2020 and the rising contribution from the new commercial operations in the USA. The number of Specialty Centers trained and accredited to administer SCENESSE® has increased to more than 40 and there are over 60 US insurers involved in the reimbursement of the cost of treatment of SCENESSE®. Expenditures continue to be well managed to support the growth of the business.
Investor Meetings
Following the release of the March quarter 2021 cash results, our senior management team, but also our scientific team met with analysts and investors. Key conference calls were held with Jefferies, UBS, Wilsons and Moelis and involved their institutional clients. Overall, we briefed more than 20 institutional investors, many of whom were new to CLINUVEL. As per usual, we answered a myriad of questions on the Company, ranging from the progress of commercial operations, all aspects of the research and development program, and the expansion of the Group. Some of the participants to the conferences were seeking separate follow-up meetings with our management team to progress their due diligence with a view to investing in CLINUVEL.
Focus on Over-The-Counter Products
There was keen focus on the complementary Over-The-Counter (OTC) product launch during the investor conferences. The rationale for flanking our medical therapies with OTC products for unserved populations seemed well understood. The OTC product lines are an initiative of CLINUVEL’s Healthcare Solutions Division to leverage the technology and expertise developed in the Pharmaceuticals Division over the years.
Information on key questions and answers provided during the analyst and investor calls, are detailed below:
| Questions | Answers |
|---|---|
| What is the approval process, regulations, and standards for non-pharmaceutical products? |
The approval process for non-pharmaceutical products is quite different to a pharmaceutical drug product. There are similarities, while our regulatory teams will be able to meet all the required standards and regulations. During the years some of the regulations and non-medical market expectations have shifted towards environmentally-friendly products. To this, we add detail on regulations in the EU and USA. In the EU, Regulation 1223/20009 is the main regulatory framework for finished cosmetic products and requires manufacturers to follow specific requirements in the safe preparation of products which must be under GMP standards. A ‘Responsible Person’ must be appointed who has specific obligations regarding the product throughout its life. Our integrated team is then tasked to oversee all aspects of the product, i.e. manufacturing, distribution and end use. There is a central register of products and rules for use of certain active and non-active ingredients, including guidelines on labelling and packaging. Of course, this is already in place for the more stringent pharmaceutical products CUV is developing and marketing. In the USA, the Food, Drug and Cosmetics Act and the Fair Packaging & Labelling Act govern non-pharmaceutical products. There is a Voluntary Cosmetic registration program and labelling requirements. |
| What are the products planned? | There will be a phased launch of a range of topical products, including four product lines in total creating added brand value. The first product line to be launched will offer polychromatic protection under extreme conditions, targeting populations at risk of solar and high energy visible (HEV) light. The second product line, assists in DNA protection and repair to populations at risk of solar damage and specific solar damage. The other product lines are not yet disclosed. |
| What are the product ingredients? | We are focused on formulations that draw on our knowledge of melanocortin molecules and chromophores to provide photoprotection and regeneration of the skin, with fragments of peptides and other anti-oxidative excipients. The product lines aim to lead topical photoprotection in the markets. We explained before that these will be launched and marketed as ‘pharmaceumables’. |
| What is the likely price range? | No price guidance has been provided at this time, although the premium products will meet assessed demand of a novel photoprotective product line in the dermocosmetics segment. |
| Where will the products be distributed? | We have not mentioned the initial countries of distribution and will provide insights upon product launch. |
| What are the consumer groups targeted? | The first product line targets populations at risk of solar and high energy visible (HEV) light insult. The second product line focuses on individuals at risk of solar damage and who require assistance in DNA repair of the skin, they are grouped as specific high-risk populations. These populations are a mix of users and patients at peril. |
| What is the planned distribution method? | CLINUVEL will reach targeted user groups using modern digital marketing methods and online purchases will be made possible. The newly established Communications, Branding and Marketing Division is critical for us to reach the targeted user groups. |
| What will be the contribution of OTC products to the Group’s revenue/profit? | The initial product launch aims to test markets while building audiences. The marketing activities will increase over time as we evaluate opportunities and establish our unique positioning within the market. We foresee that demand for the product lines will gradually occur. CLINUVEL is progressing this new business line deliberately to grow with a clear and considered plan. Initially, we believe the healthcare or personal care business will complement the Group’s current earnings rather than eclipse these of the core Pharmaceuticals Division. It will however, cement our positioning as experts in the field of systemic and topical photoprotection, where opportunities for expansion are clear. |
| Will the OTC products cannibalise the pharmaceutical drug market? | No, of course not, the non-pharmaceutical products can never be substitutes for the medicinal efficacy of pharmaceutical drugs required as a therapy for severe indications. Our systemic solutions work from within, our topical solutions from outside inwards. Both complement each other. |
I am explaining in all our investor and analyst meetings that all our new investors would surely appreciate that the Company needs to balance the disclosure of plans and details of product launch against the early extensive release of information, which could be used by competitors seeking to move ahead of CLINUVEL’s entry to the dermocosmetic market. We will provide more information on the product launch as we progress and advise when there are further updates on the OTC Product Launch.
CLINUVEL is Reported to be “One of the Fastest Growing Companies in Asia Pacific”
In April 2021, CLINUVEL was included in the High-Growth Companies Asia Pacific 2021 ranking. Compiled by the Financial Times, Nikkei Asia, and Statista, the top 500 fastest growing companies in the region, spanning 13 countries, were ranked by their compound annual growth (CAGR) between 2017 and 2020. CLINUVEL ranked 351st with a CAGR of 24.2% and was one of 71 Australian companies included in the list. The countries with the most companies in the list were Japan (116), India (95) and Singapore (72). Only 11 companies were from the pharmaceutical sector, making CLINUVEL’s achievement even more notable. Independently of the list, the Financial Times published an article on CLINUVEL on 16 April.
Conference Events
We participated in the UBS Global Healthcare Virtual Conference on 24 to 26 May and are presenting to the Jefferies Virtual Healthcare Conference on 03 June. As has been the norm in 2020 and 2021, both are held virtually while hosted from New York. Selected meetings with interested investors have been scheduled at both conferences. Dr Wolgen’s fireside chat on 03 June with Dr David Stanton of Jefferies will be a highlight, providing an overview of the Company’s history and plans.
As per usual, the calendar of planned events for 2021 is provided below as information, noting a number are yet to be confirmed.
| Month | Planned Events |
|---|---|
| January |
JP Morgan Healthcare Conference, San Francisco |
| March | Daiwa Investment Conference, Tokyo |
| May |
UBS Global Healthcare Virtual Conference |
| June |
Jefferies Virtual Healthcare Conference |
| September |
Goldman Sachs European Medtech & Healthcare Conference (tbc) |
| October |
Morgans 5th Annual Value in the Vines Investor Conference (tbc) |
| November |
Jefferies London Healthcare Conference (tbc) |
Conclusion
The CLINUVEL business case continues to hold the fascination of all involved, our patients, prescribers, staff and Board of Directors; the story is gripping not in the least due to the possibility of the biological response of our technologies in new and widely relevant indications. Amidst changing markets and macro events exerting influence on our business, the CUV team is putting minds towards diversification yet totally committed to the single outcome of making CUV a standout pharmaceutical and healthcare business. The clinical success to date does not make us impervious to possible future disruptions, set-backs or new economic foes and therefore, we remain realistic and determined to build the Group outwards.
At each station, I question whether the expedition succeeds in reaching its next base camp, K2, a part of that very piquancy. We keep moving forward until our chartered summits are reached, no matter how difficult and irrespective how the odds are stacked in development, distribution and market access.
We invest time, energy and resources on our staff as a repository of knowhow, particular skills and experience bundled in one group spread over 7 locations; for this there is a strong call for discipline and incessant communication among us. Drawing on this talent pool, we need faster decision moments to operate in a new world. Our Board is steadfast in its goals to create a premise for long-term success and in unity, we bear the patience to see all developments progressing towards a specialty pharma in melanocortins.
The last quarterly figures reported on 29 April underscored steady progress. The Company’s financial basis invites further expansion and allows us to recruit specialised professionals. On the back of a widely acknowledged prospect of a post-Covid market surge, we work through the obstacles, rely on our health, common sense and look to build our construct on several pillars.
The opening touched on the factors binding this CUV team, and most appropriately I finish with the same theme, since it does impact how we operate and the calibre of new investors CUV attracts. More than a decade ago, the decision to run an organisation which had missed its objectives during previous decades was a conscious one, since I envisioned a focused team on human sciences. Years later as society evolves, we ask ourselves more than before “what is it that matters exactly?” Former Governor of the Bank of England Mark Carney questioned markets’ activities to serve self-interest, and I am unsure whether this label is still current. I predominantly see signs of market participants looking for their funds to be allocated towards a much broader definition of value.
In April, and with much interest I learned from new German investors how they spoke about supporting a predictable entrepreneurial team providing tangible benefit to society, patients. These investors expressed a willingness to bear the investment risk as long as they understood that the company was spending funds in a cost-conscious manner on worthwhile causes. This occasional discourse is rich, as one learns from select group of investors how their decisions are made on past performance and attitude.
This liberal shift in money allocation is on a larger scale relatively new. Although we have known for decades the activity of socially responsible investing, there is a wider movement of putting money towards preferred causes and people managing it. Where Carney is correct though is in his views on the axis between value and values, a theme akin to CLINUVEL in light of its expansion. I know where much of CLINUVEL’s current success finds its grounding, and a usable barometer is by asking new candidates interviewing for a position why they had applied. In a great majority of cases the uniform answer is that it is CUV’s values and vision that make the professionals want to jump ship.
It is on us now to coalesce that very essence into a sustainable group, innovating at present more than a dozen realistic projects generating equity for all beneficiaries.
I appreciate you all for your continued support.
Philippe Wolgen
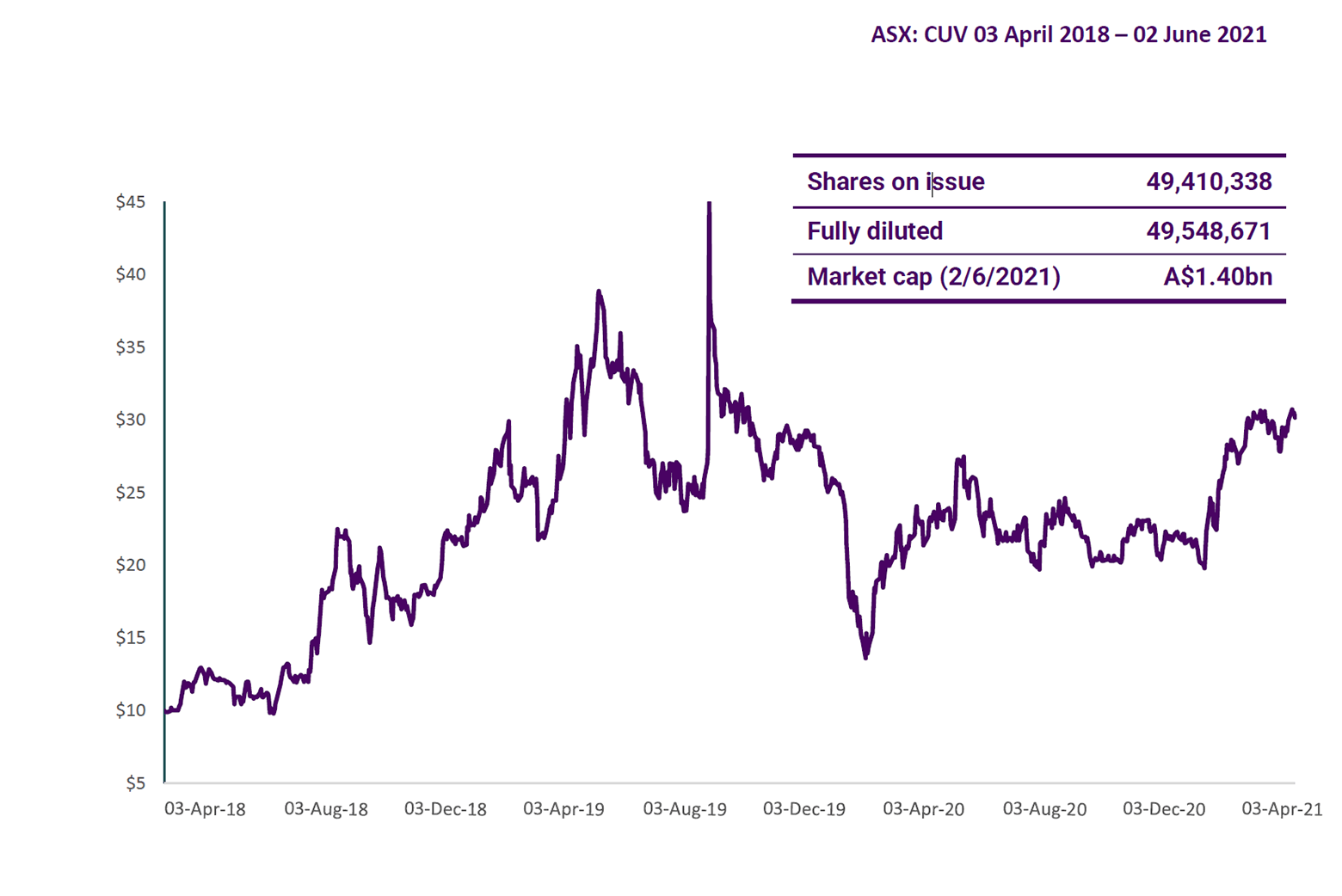
Share Price
Authorised for ASX release by the Board of Directors of CLINUVEL PHARMACEUTICALS LTD.
Forward-Looking Statements
This release contains forward-looking statements, which reflect the current beliefs and expectations of CLINUVEL’s management. Statements may involve a number of known and unknown risks that could cause our future results, performance, or achievements to differ significantly from those expressed or implied by such forward-looking statements. Important factors that could cause or contribute to such differences include risks relating to: our ability to develop and commercialise pharmaceutical products, the COVID-19 pandemic affecting the supply chain for a protracted period of time, including our ability to develop, manufacture, market and sell biopharmaceutical products; competition for our products, especially SCENESSE® (afamelanotide 16mg); our ability to achieve expected safety and efficacy results through our innovative R&D efforts; the effectiveness of our patents and other protections for innovative products, particularly in view of national and regional variations in patent laws; our potential exposure to product liability claims to the extent not covered by insurance; increased government scrutiny in either Australia, the U.S., Europe, China and Japan of our agreements with third parties and suppliers; our exposure to currency fluctuations and restrictions as well as credit risks; the effects of reforms in healthcare regulation and pharmaceutical pricing and reimbursement; that the Company may incur unexpected delays in the outsourced manufacturing of SCENESSE® which may lead to it being unable to supply its commercial markets and/or clinical trial programs; any failures to comply with any government payment system (i.e. Medicare) reporting and payment obligations; uncertainties surrounding the legislative and regulatory pathways for the registration and approval of biotechnology based products; decisions by regulatory authorities regarding approval of our products as well as their decisions regarding label claims; any failure to retain or attract key personnel and managerial talent; the impact of broader change within the pharmaceutical industry and related industries; potential changes to tax liabilities or legislation; environmental risks; and other factors that have been discussed in our 2020 Annual Report. Forward-looking statements speak only as of the date on which they are made, and the Company undertakes no obligation, outside of those required under applicable laws or relevant listing rules of the Australian Securities Exchange, to update or revise any forward-looking statement, whether as a result of new information, future events or otherwise. More information on the forecasts and estimates is available on request. Past performance is not an indicator of future performance.
