SCIENTIFIC COMMUNIQUÉ X: Photoprotection and the significance of Minimal Erythema Dose (MED) testing
May 2021
ABSTRACT
The sun continuously emits radiant energy across the solar spectrum, which includes ultraviolet (UV) radiation. Frequent overexposure to UV radiation is the main cause of premature ageing (photoageing) and the cause of over 90% of all skin cancers. Globally, we have reached a new peak in the number of skin cancer cases being diagnosed every year. The World Health Organization (WHO) reports skin cancer as the fifth most common form of cancer, although in many countries, including the US and Australia, it is the most common cancer.
Photoprotection – protection from the damaging effects of light, including UV radiation – is the mainstay of skin cancer prevention. More robust photoprotective measures are being developed, however, the question arises: how do we measure the effectiveness of these agents?
UV stimulates a series of morphological (structural) and genomic changes within the cells of our skin which contribute to the known long-term adverse effects of frequent unprotected sun exposure. Some of these cutaneous alterations are palpable to the naked eye just hours after moderate to intense UV exposure, others take many years to manifest. Sunburn, otherwise known as solar erythema, is an acute response to UV radiation and is a reaction that has been exploited in the field of photomedicine as a means to quantify photosensitivity.
Minimal Erythema Dose (MED) is a measurement used regularly to examine skin tolerance to UV in the clinic and within experimental studies. Specifically, MED is a quantification of the threshold dose required to stimulate the signs of solar erythema. It is used primarily to determine sun protection factor (SPF), calculate suitable doses for light therapy and during the diagnosis of photoreactive disorders (phototesting). Significantly, and relevant to CLINUVEL’s focus, in recent times, MED has also had a suggestive role as a non-invasive alternative to other common clinical approaches to estimate DNA damage.
The ease and practicality of MED has made it an attractive measurement for research, however, when utilising this technique precautions must be made to ensure its accurate and precise use. Evaluating contemporary photoprotection also may extend from the capabilities of current MED testing, therefore suggesting the need for supplementary examinations.
INTRODUCTION
The sun’s energy is constantly surrounding us, even if we cannot always see it. Collectively known as the solar spectrum, this energy can be broken into three distinct wavelengths: ultraviolet (UV) radiation (100-400 nm), visible light (380 to 700nm), and infrared radiation (780 – 1000nm). While essential for all forms of life, the sun’s energy has numerous harmful effects on our skin, particularly when we are overexposed to it on a regular basis.
In over 90% of all skin cancer cases, overexposure to the sun and other artificial sources of light are the known causes, with global incidence of disease continuing to increase. In Australia alone, almost 980,000 new cases of non-melanoma skin cancers are treated each year, with more than 13,000 individuals diagnosed with melanoma. Tragically, skin cancers are responsible for an estimated 2,000 Australian deaths per annum. In parallel to the human burden, the financial impact of skin cancer also weighs heavily on healthcare systems. The cost for the diagnosis and treatment of non-melanomas alone exceeded an estimated A$703 million in 2015. This figure excludes treatment costs of new cases of melanomas, which was reported at A$201 million in 2017. The increase of these costs in 2021 is estimated to have escalated to more than A$1 billion in direct treatment excluding the loss of employment and productivity. Similar trends of financial burden have been matched in many other countries including the US, UK and across Europe (Table 1).
| Country | Population | Total health expenditure cost of malignant melanomas (A$) |
|---|---|---|
| United Kingdom | 63, 700, 300 | 90, 929, 603 |
| Italy | 59, 539, 717 | 57, 471, 458 |
| Germany | 80, 425, 823 | 148, 435, 208 |
| France | 65, 659, 790 | 84, 134, 290 |
| Switzerland | 7, 996, 861 | 40, 549, 918 |
| Norway | 5, 018, 573 | 25, 886, 757 |
| Denmark | 5, 591, 572 | 28, 680, 627 |
Table 1: Health expenditure costs for malignant melanoma in European countries in 2015.
Though less harmful, sun damage is also the main cause of premature signs of ageing skin (wrinkles, hyper-pigmentation, and discolouration), otherwise known as photoageing. In fact, 80% of skin ageing, meaning loss of elastin and collagen, results from photoageing. While some may exclude this process as a purely a cosmetic problem, it is a visible sign that our skin’s normal functions have been corrupted. The ability for skin to initiate wound healing, for example, is considerably reduced in individuals with photoaged skin, subsequently enhancing their risk for infections.
Understanding the cause of photodamage and photoageing has given the scientific community an advantage when developing essential and preventative treatments. Yet effective methods by which therapies be assessed and compared are paramount to the success of developing novel protective therapies. In this communiqué, we examine the application of one of these assessment methods: Minimal Erythema Dose (MED). We will review its use, advantages, and identify potential downfalls which may impact its viability in quantifying or measuring photoprotection. We will also look at the pertinence of MED in relation to DNA damage which has become a current topic of discussion in modern research.
HISTORY OF MEASURING PHOTOPROTECTION
Swedish physician Erik Johan Widmark was one of the first scientists to hypothesise that UV radiation from the sun had strong and harmful effects on the human body. In 1889 Widmark tested his theory, placing a quartz plate on top of his skin, a material known to filter out the longer wavelengths of the solar spectrum. After prolonged exposure to the sun, he noticed an acute reaction appear – solar erythema (sunburn; see Annex 1). This was a crucial insight that gave rise to a new understanding of light’s interaction with man, one which had previously gone largely unnoticed. It was now clear that intense UV exposure was capable of causing almost immediate changes to the skin, visible to the naked eye. Years later, this knowledge would be captured and harnessed to create a useful and longstanding clinical assessment tool: MED¹.
By the early 1900s, further scientific research had characterised skin cancer as a prominent effect of chronic sun exposure, and medical efforts focused on building awareness of this connection and protecting individuals from harm.
Photoprotection is defined as a method to prevent the development of sun-induced acute and chronic actinic damage. While it comes in many different forms (clothing, behaviour and even education around sun safety) the most common form of photoprotection is the use of topical sunscreens. The first modern sunscreen was developed by an Australian chemist, Milton Blake, who created his ‘photoprotective creams’ soon after awareness around sun damage began to gain traction. Cultivated in pots and pans in his home kitchen, he launched the product commercially in 1928 as a defensive concoction against sunburns.
Blake, however, was not the only chemist working on creating a topical form of photoprotection. By the mid-1900s there was a sudden boom in the number of lotions and ointments claiming sun protection. However, there was no definitive way for consumers to distinguish between the shielding effects of one product to the next. German physicist Rudolf Schulze set to the task of identifying a solution.
MED is a representation of an individual’s sensitivity to light radiation. It is the lowest dose of UV radiation required to cause the perceivable sign of erythema, which is observed as reddening of the skin. In 1956, Schulze realised that an increase in a patient’s MED, following treatment with sunscreen, would prove product protection against sun damage based on its ability to delay or extend the onset of our skin’s erythemal response. The “Schulze Factor”, a formula that became the first standardised method of evaluating topical photoprotection, was born. Though not its first use, the Schulze Factor was one of the earliest widespread applications utilising MED testing for commercial purposes. In 1974, the Schulze Factor was renamed Sun Protection Factor (SPF) by Austrian chemist Franz Greiter, as he started to use this formula to champion the efficacy of his own sunscreen creations. (Figure 1).
¹MED is the minimal dose of UV radiation (J/cm2) required to produce the first perceptible unambiguous erythema (redness on the skin) with defined borders appearing 24 hours after irradiation. In simplistic terms, it is a measure of an individual’s tendency to burn, with low MED values associated with increased photosensitivity.
SPF=
(MED = minimal erythemal dose)
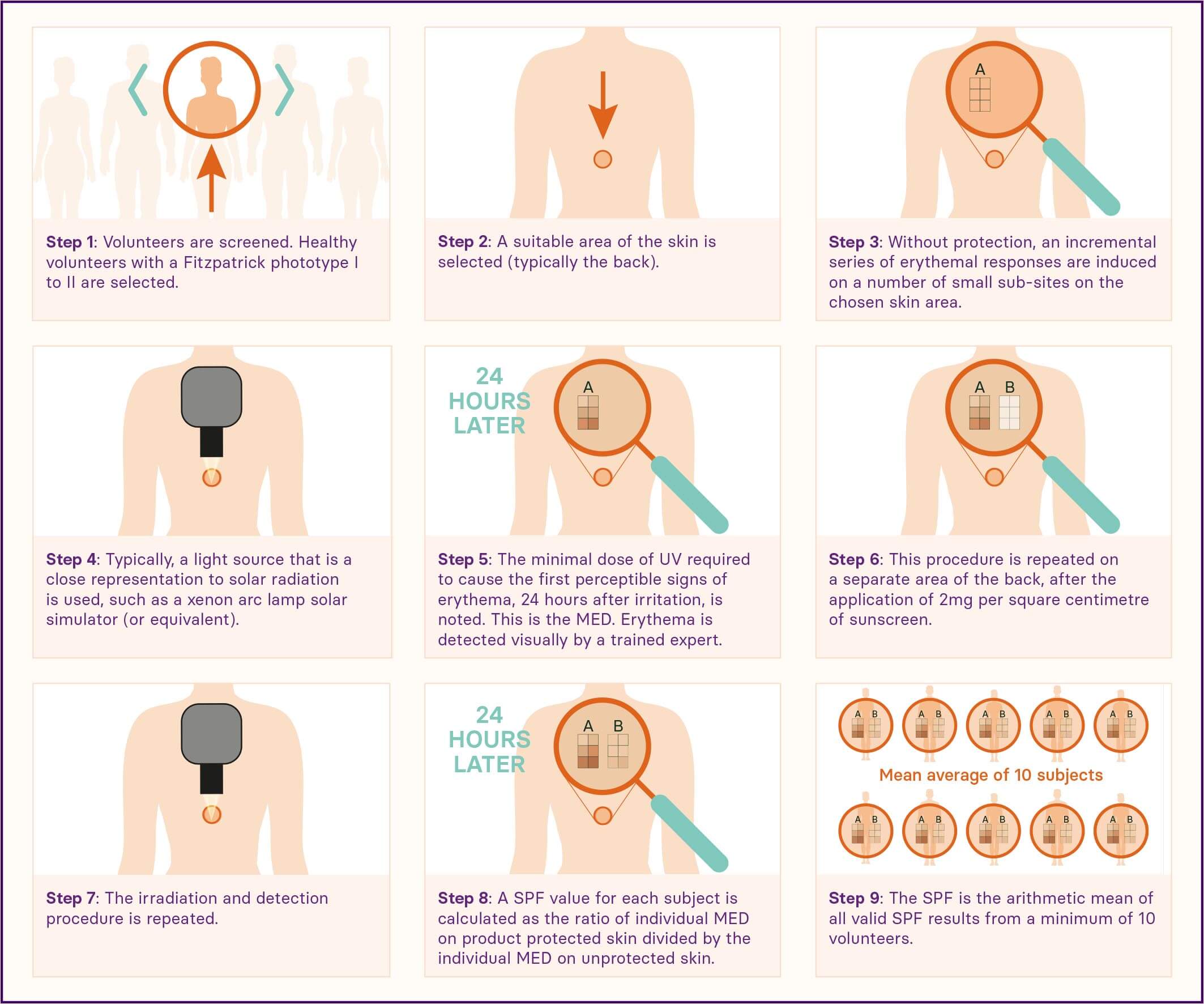
Figure 1: Simplified formula for calculating sun protection factor (SPF). The minimal dose of UV radiation required to induce the first perceptible signs of erythema on unprotected skin is measured after 24 hours following irradiation. A second area of the skin is then treated with a standard amount of the product (2 mg per square cm of the final sunscreen formula) and the process repeated. The MED of protected skin is divided by the MED of unprotected skin and the calculated value is the SPF rating. The greater the MED on protected skin in relation to the MED of the unprotected skin would be suggestive of a higher product efficacy against sun damage as the minimal dose required to stimulate erythema increased by a larger amount after the application of sunscreen application. Overall, SPF is evaluating how effective a product is at reducing UVB induced sunburn.
The rebranded SPF soon became popularised and was the only measurement that described a sunscreen’s protective abilities, used worldwide by chemists and dermatologists alike. Interestingly, most of these earlier sunscreens only had low SPFs, ranging mostly from 2 to 4. Products were labelled to provide ‘maximal photoprotection’ if their calculated SPF exceed 8 (which regulatory bodies now consider almost ineffective against reducing an individual’s skin cancer risk). Due to the lack of control around conducting MED initially, however, the stated SPFs also varied considerably. Schulze’s way of measuring MED was crude but there was value in SPF certification, and MED testing was a viable tool as to determine it. Thus, an effort was placed upon improving and validating this new practice. In 1978, the US Food and Drug Administration (FDA) proposed the first guideline to determine SPF and, in 2006, the International Global Harmonized SPF method was created which synchronised national MED testing and attempted to certify consistency between worldwide laboratories. The International Standards Organization (ISO) and FDA now publish the current standardised methodologies which are utilised by most.
CALCULATING SPF THROUGH MED
The SPF test method is now a laboratory-based method that utilises a solar simulator (a device emitting UV energy) to determine the protection provided by sunscreen products on human skin against erythema. The general principle of the method is reviewed in Figure 2.
ADVANTAGES OF MED TESTING
SPF remains the main determinant of sunscreen efficacy some 70 years after its introduction to photodermatology. We often hear SPF and sunscreens used interchangeably, demonstrating its automatic association with photoprotection, and thus substantial and successful uptake.
This is, in part, because the MED technique used to determine SPF has significant practical advantages. Performing MED is first time-efficient, minimising delays and enabling patients to access new and potentially life-changing treatments. Erythema, as an endpoint, is also easy to detect yet remains clinically relevant as there is a known link between recurrent sunburns and an increased risk for melanoma (see Wu et al, 2016). It is a cutaneous change that can be induced in almost all individuals, unlike other sun-induced skin alterations. The doses used to stimulate erythema are also low, with the MED method associated with minimal adverse events. This overcomes ethical challenges introduced by other parameters of sun damage.
Measuring MED is also simple. It can be accomplished using cost-effective equipment which is commercially available and requires only basic laboratory skills. The simplistic nature of MED testing means it can also be used in other areas of general dermatology too, with its current uses also including phototesting and determining safe dosing during phototherapies.
Other practices have attempted to quantify photoprotection outside of SPF, yet global consensus has not been achieved by these newer methods. Overall, SPF and the MED tool has driven the discovery and development of innovative UV filters that have helped in the fight against rising skin cancer rates.
MINIMISING VARIABILITY
MED testing has been subject to some scrutiny over the years. A 2016 publication from the Consumers’ Institute of New Zealand, for example, highlighted significant differences in SPF results following sunscreen analysis in numerous independent clinical laboratories. The report noted almost 50% of the products they assessed failed to meet label claims, inferring the unreliability of MED testing.
The discrepancies discussed can be, in part, blamed on the high sensitivity of the MED methodology. A large number of variables must be tightly controlled during the procedure, thus while the tool is useful, results are easily skewed by minor changes that may unintentionally occur during its execution. Originally utilised almost a century ago, the initial design of the MED procedure was basic, consistent with the technological advances of the era. Experts have therefore placed time and effort upon first identifying the cause of reoccurring errors and then formulating suitable solutions to combat these faults to enhance the precision, and therefore usability of this technique.
One such improvement has included removing the subjectivity of erythema recognition. Several decades ago, the effects of UV radiation was merely, and inexpertly, distinguished by the naked eye and without the need for technical apparatus. Over time as its use became customary, multipoint rating systems, such as the Likert-type visual rating scale, were introduced in an attempt to further heighten the precision of erythema detection. Though this was an improvement, visual assessment of ‘just-discernible’ erythema was, however, still error-prone. What appeared as the signs of erythema to one examiner was not necessarily detected by another. Diffey and Robson (1992) reported accurate readings were, at times, hard to produce due to difficulties in recognising reddened skin in the presence of varying amounts of pigmentation especially in subjects with darker skin tones. In recent years, laboratories have begun to incorporate the use of spectrophotometers. Spectrophotometers can perceive subtle changes in skin colour, including redness, which are almost undetectable with the naked eye, removing the subjective determination of examiners. Using this instrument to measure superficial responses to UV radiation thus has the added benefit of reducing the amount of UV radiation required to produce a perceptible change. In turn, this increases the safety of the tool by reducing risks such as those seen with (both acute and chronic) excessive irradiation. While the 2019 ISO guidelines still refer to the visual judgment of erythema, this is expected to change in upcoming revisions.
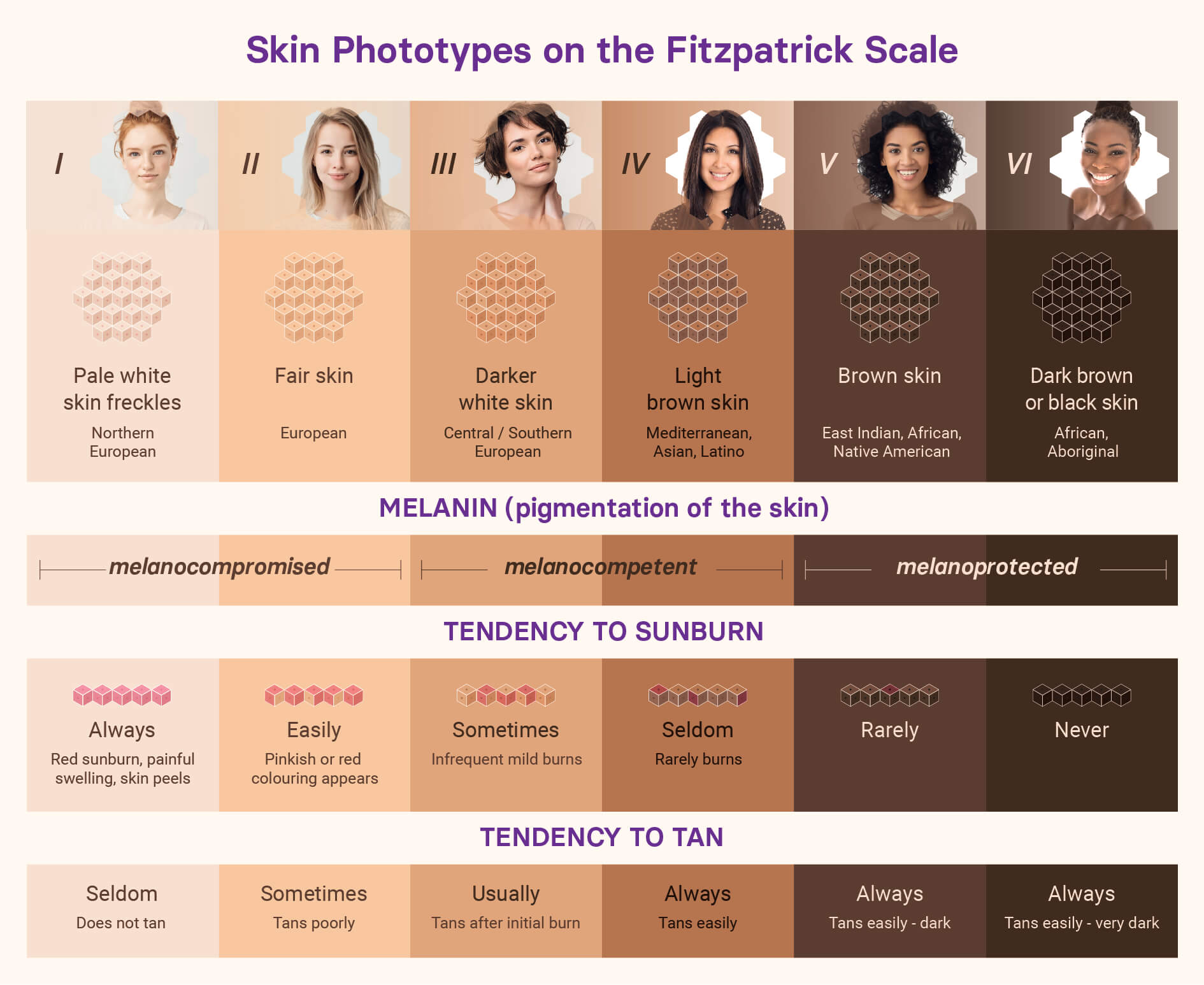
In conjunction with Diffey and Robson’s observations, Damian et al (1999) noted that measuring SPF using patients with phototypes associated with fairer skin (or lower MEDs) resulted in higher final SPF values. They highlighted that a strong negative correlation exists between constitutive pigmentation and erythemal responsiveness. The concentration of eumelanin, the black-brown photoprotective pigment found naturally in healthy skin, fluctuates significantly between individuals. Inversely associated with skin phototype, those living with a darker complex, or Fitzpatrick phototype IV to VI, will have a greater innate resistance to the harmful effects of the sun, including erythema, as a result. In general, we now understand that MED increases by steady increments between each sequential Fitzpatrick phototype (Figure 3).
The selection of volunteers for SPF studies thus plays a role. During commercial SPF determination, only individuals with Fitzpatrick phototype of I to III are recruited. This is mainly due to time constraints, as erythema is generated more rapidly, and arguably more visibly, in these subjects. While this is also an attempt to harmonise test conditions globally, a study that recruits mostly individuals with Fitzpatrick phototype I, for example, will thus still report a higher SPF of a given product than if all volunteers were classed as Fitzpatrick phototype III. To complicate matters further, self-reports are used to determine Fitzpatrick phototype and photosensitivity, introducing further potential biases. The heterogeneity in reported SPFs, as highlighted by the Consumers’ Institute of New Zealand, may be a consequence of the variations in phototyping and the effect it therefore has upon SPF calculation. Consistency is key to minimise this potential issue. Although the ISO states to use volunteers with skin type defined as Fitzpatrick I to III, experts have instead suggested, the use of equipment which can non-objectively define skin pigmentation. One such example is the use of Individual Typology Angle (ITA°), a reflectance measure of one’s skin pigmentation based upon colourimetric parameters, measured by a chromameter. Defining phototype by an individual’s ITA° and setting defined inclusion and exclusion criteria for subject recruitment based upon ITA° values may increase accuracy in SPF determination.
Other factors can influence the measurement of MED. The location of irradiance, presence of moles, hair or blemishes, presence of sweat (as a thermoregulator) and gender of study participants have all been shown to skew MED (and thus SPF) results. While the ISO has made attempts to standardise light sources, there is also great variance in the globes and solar simulators used for MED testing, meaning subjects are irradiated with different combinations of UVB and UVA wavelengths which has a direct influence on the ease of erythema induction. Light sources may also fatigue over time, especially after prolonged use, gradually lowering irradiance intensity and therefore distorting results.
The ISO collaborates with expert working groups to continuously improve the MED testing procedure, reviewing current policies every five years. Many of the issues outlined, for example, have already been flagged and are due to be incorporated into the forthcoming ISO SPF guideline. Not all countries, however, have adopted the ISO guidelines. The USA and Taiwan for example, are following alternative recommendations. Furthermore, ISO standards are not mandatory. Results collated from industry or within a clinic that has not followed a recognised and certified guidance procedure should be reviewed cautiously.
In short, greater consistency in approach is not only key but needed. It is hoped that this will result in more accurate SPF ratings and better information being provided to a sunscreen used by the public.
MED, A SPECTRAL SURROGATE FOR DNA DAMAGE?
With MED testing demonstrating its beneficial use in general dermatology and during commercial SPF testing, research experts have begun to consider its use in more advanced settings. Conversations have arisen around whether MED testing could become a more permanent and routinely used tool in investigational research, especially in the field of oncology.
When our skin comes in contact with light, the DNA of our skin cells are almost immediately damaged. The extent of the damage will rely on several factors such as time of exposure, light intensity, and our body’s ability to recognise and repair our DNA. This change, however, can be the cause of carcinoma development if left to become “permanently fixated” within our genome (see SCIENTIFIC COMMUNIQUÉ VI).
Understanding and having the ability to quantify the level of DNA damage is extremely significant in today’s medicine. As society migrates towards a personalised approach to healthcare, understanding individual susceptibility to skin cancer will have major advantages when developing both preventive and potentially reverse treatments.
Assays established to measure DNA damage are complex and, in most circumstances, require the use of skin biopsies. This invasive procedural requirement complicates both recruiting and evaluating human subjects as it introduces ethical hurdles.
Furthering the challenge, these biopsies are then analysed for biomarkers for DNA damage, which often requires expensive and complicated equipment for which technical expertise is essential. The equipment and necessary manpower are not readily available in all laboratories.
It is these drawbacks that have spurred new ways of thinking about MED and its value as a clinical assessment tool. MED is primarily measuring an individual’s tendency and time to burn, but could it also be used as an indirect and safer way to examine DNA damage?
²XP results from a deficiency in the body’s normal repair system against UV induced DNA damage. Compared to the general population, these patients show a significant accumulation of genomic damage that, in turn, eventually turns skin cells cancerous. It is suggested that the high extent of DNA damage in these patients is, at least partially, responsible for the emphasised erythemal responses to UV light.
Erythema presents itself as a secondary consequence of cutaneous DNA damage (Annex 1). This suggests a biological coherence between DNA damage and erythema which is further corroborated by a known link that exists between the number of sunburns and increased skin cancer risk. From this alone, there is a hint that the signs of erythema, as detected through MED testing, are directly related to the level of DNA damage. Extending this notion, patients with the genetic disease xeroderma pigmentosum (XP)² can show abnormal and exaggerated erythema responses after exposure to sunlight or other artificial sources of UV radiation. Both these facts show there is significant theoretical evidence to suggest that erythema could serve as a non-invasive clinical surrogate for biopsies to help measure DNA damage.
This hypothesis was shared by a study group led by Young et al (1998). After investigation, he reported the action spectra required to cause both maximal genomic damage and erythema were extremely similar, with the peak of UV-induced carcinogenicity shown to be within the UVB and UVAII portion of the sunlight spectrum. At wavelengths greater than UVAII (>340 nm), and thus a range of energy outside the amount required for erythemal induction, the number of thymine dimers (a type of DNA damage caused by the sun) in the skin cells of the clinical subjects fell significantly. It was concluded that erythema was a good spectral surrogate for the UVB and UVAII component of sunlight-induced DNA damage.
More recently, Kohli et al (2017) also found a positive linear association between erythema intensity and UVB doses independent from Young’s experiments. This study was examining the photoprotective efficacy of a systematic antioxidant against molecular damage. He used several methods to determine this, one of which was a change in a subject’s MED. An increase in MED correlated with the drug’s ability to minimise DNA damage, confirmed by alternative assays. Kohli concluded that colourimetric examination of erythema could therefore substitute for directly measuring DNA damage.
A handful of other research groups, including Miller et al and Heenen et al, described similar correlations in their own findings to the prementioned studies but, while it is clear that a relationship between these two endpoints may exist, further comparable literature is required before a conclusive remark can be made. These additional experiments should involve larger and more statistically significant patient pools. At this present time, in the field of photo-quantification, MED testing is only FDA approved for the determination of SPF ratings.
EVOLVING KNOWLEDGE OF PHOTODAMAGE
Compared to several decades ago, we are now aware sun damage is not limited to the effects induced by solar UV radiation. The pathology of erythema is caused predominantly by UVB radiation, which excludes the genomic damage induced by the longer wavelengths of the solar spectrum (including a large portion of UVA radiation). In the case of UVAI (340 – 400 nm) and HEV light (the violet-blue portion of the visible spectrum, 380 – 500 nm), erythema is not observed, despite the known occurrence of DNA damage. Therefore, forms of photoprotection that aim to examine efficacy outside the UVB range may not benefit from MED testing. Instead, alternative endpoints, such as pigmentary changes, could be swapped for erythema.
CONCLUSION
Due to its tangible and identifiable characteristics, erythema is a useful indicator for the occurrence of photodamage, which can be easily recognised in the clinic. Its rapid induction eases the measurability of skin damage, especially when compared to other visible endpoints of photodamage, such as skin cancer or photoageing. MED, therefore, exists as a valuable non-invasive tool to approximate the intensity of sun-induced damage inflicted upon our skin by sources of UV radiation. This makes its use in general dermatology, including quantifying topical sunscreens through SPF, highly useful. With the global sun care industry valued at an estimated $11.6 billion in 2018, MED testing has no doubt become indispensable in the field of photomedicine. It remains recognised by both dermatologists and consumers worldwide as the dominant methodology to calculate photoprotection, despite several alternative practices now existing. It must be emphasised, however, that the methodology for MED requires further fine-tuning to reduce variations seen in SPF results.
Based on the clear advantages of the MED method, the scientific community have started to assess the application of erythema as a surrogate for DNA damage. While it is still largely up for debate, there is mounting evidence to suggest a concordance between the intensity of erythema and the level of UVB induced DNA damage. Being able to quantify the level of cutaneous DNA damage is critical for the development of more effective forms of treatments or preventive strategies against both melanomas and non-melanomas. It also gives physicians an understanding of an individual’s risk for skin cancer. Determining whether this simple process may yield yet further benefits in evaluating photoprotection is therefore a topic worthy of pursuing. As the company continues its ground-breaking work on systemic and local forms of photoprotection, understanding the relevance of tools such as MED are critical to the group’s work.
Annex 1
A sunburn is one of the main acute alterations that takes place within our skin following overexposure to UV light, alongside melanogenesis (tanning) and skin thickening. Induced primarily by UVB (280 – 320 nm) and UVAII radiation (320 – 340 nm), it is an inflammatory reaction that can be divided into several steps.
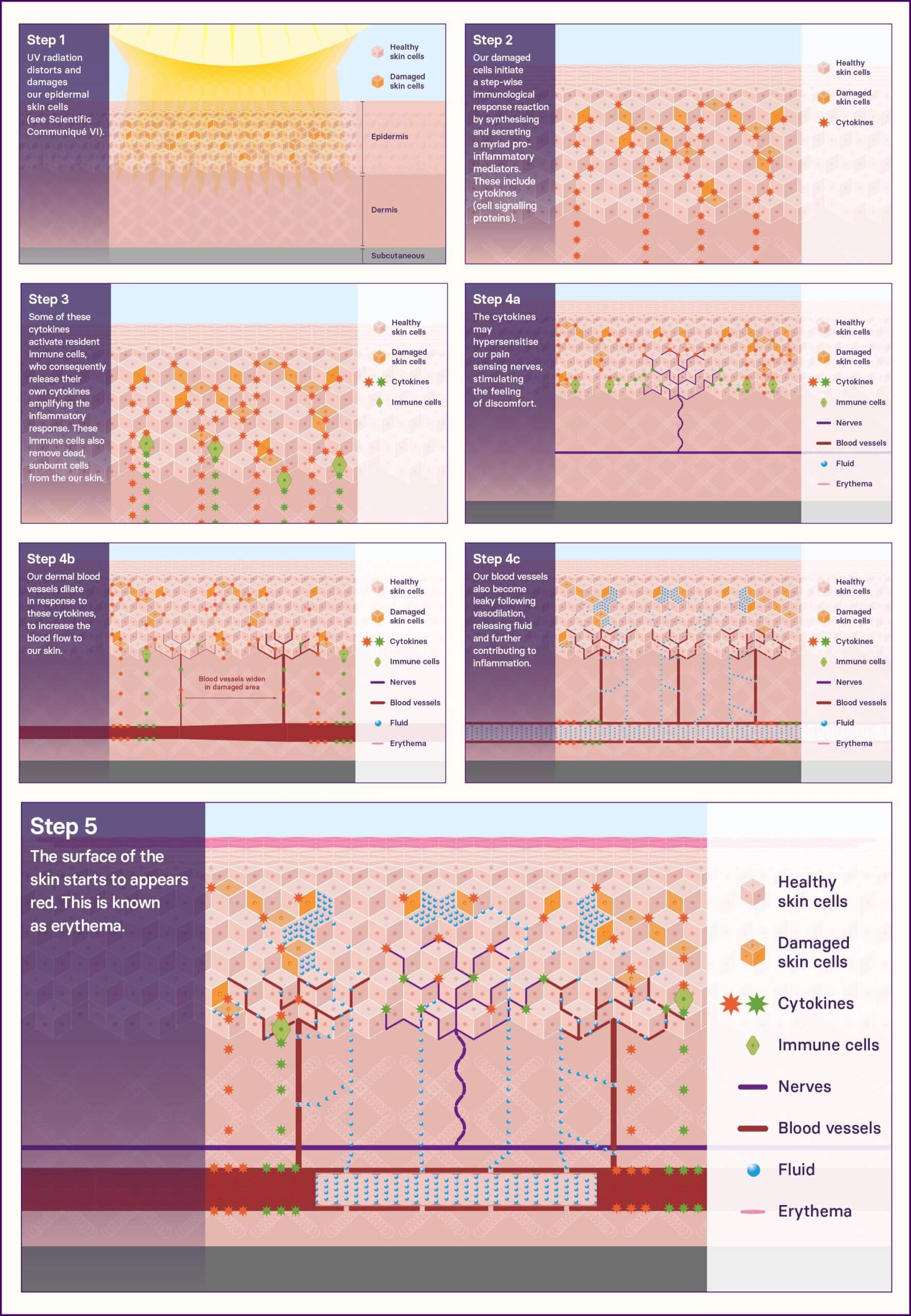
UV radiation directly excites and distorts the DNA of our skin cells found in the upper layers of the skin (epidermis), generating an abundance of photolesions. It is these lesions that can transform into permanent and, potentially, carcinogenic mutations, the precursor event to skin cancer development (see SCIENTIFIC COMMUNIQUÉ VI). UVB and UVAII can also react with other molecules within our skin to generate large quantities of reactive oxygen species (ROS). ROS breaks down essential structures of the cell. In extreme cases, the affected skin cells cannot recover from the impact which causes them to undergo cell death (apoptosis). [STEP 1]
Together, these events collectively initiate a stepwise immunological response reaction. Our damaged skin cells synthesise and secrete myriads of pro-inflammatory mediators. These include cytokines (cell signalling proteins). [STEP 2]
Resident in the surrounding tissue are dormant immunological cells, including our mast cells and macrophages, which become activated upon stimulation by cytokines and ROS. Similarly, these immune cells also release their own pro-inflammatory mediators, which not only further amplify the damage signal from the keratinocytes, but work to recruit more immune cells from surrounding tissue and the blood. These immune cells have a number of roles, including removing apoptotic (dead) sunburnt cells, minimising infection from opportunistic microorganisms and helping instigate the healing process. [STEP 3]
An individual may start to experience the first signs of physical discomfort as these cytokines hypersensitise local nociceptors, commonly known as our pain-sensing nerves. [STEP 4a]
Vasodilatory agents, such as nitric oxide (NO) are also released by both the damaged skin cells and the immune cells. These molecules exert their function upon the skin’s vasculature system that lies embedded within the dermis layer of the skin. In response, the blood capillaries expand as they are consigned to a state of relaxation. [step 4b]
Local cutaneous blood flow is increased by roughly 3x the normal amount [STEP 4c] which is observed as reddened skin (solar erythema), which is warm to the touch. [STEP 5, overleaf]
Erythema has one main purpose: to increase oxygen and nutrient perfusion to the damaged area in an attempt to nourish the vulnerable layers of the skin and promote recovery. Permeability from the microvasculature also rises, which is a consequence of both vasodilation and immune cell extravasation from the blood and into the tissue.
REFERENCES
Abhishek, K., & Khunger, N. (2015). Complications of skin biopsy. Journal of Cutaneous and Aesthetic Surgery, 8(4), 239–241.
Australian Bureau of Statistics. Causes of Death, Australia, 2017. Vol. 3303.0. Australian Bureau of Statistics: Canberra, Australia, 2018.
Barnes, P. W., Williamson, C. E., Lucas, R. M., Robinson, S. A., Madronich, S., Paul, N. D., Bornman, J. F., Bais, A. F., Sulzberger, B., Wilson, S. R., Andrady, A. L., McKenzie, R. L., Neale, P. J., Austin, A. T., Bernhard, G. H., Solomon, K. R., Neale, R. E., Young, P. J., Norval, M., … Zepp, R. G. (2019). Ozone depletion, ultraviolet radiation, climate change and prospects for a sustainable future. Nature Sustainability, 2(7), 569–579.
Cancer Council Australia, 2021. 2021-2022 Pre-Budget Submission.
Clydesdale, G. J., Dandie, G. W., & Muller, H. K. (2001). Ultraviolet light induced injury: Immunological and inflammatory effects. Immunology & Cell Biology, 79(6), 547–568.
Diffey, B. L., Jansén, C. T., Urbach, F., & Wulf, H. C. (1997). The standard erythema dose: A new photobiological concept. Photodermatology, Photoimmunology & Photomedicine, 13(1–2), 64–66.
Heenen, M., Giacomoni, P. U., & Golstein, P. (2001). Erythema, a link between UV-induced DNA damage, cell death and clinical effects? In Comprehensive Series in Photosciences (Vol. 3, pp. 277–285). Elsevier.
Huang, M.-W., Lo, P.-Y., & Cheng, K.-S. (2010). Objective Assessment of Sunburn and Minimal Erythema Doses: Comparison of Noninvasive In Vivo Measuring Techniques after UVB Irradiation. EURASIP Journal on Advances in Signal Processing, 2010(1), 483562.
ISO-24444-2019, 2019, Cosmetics — Sun protection test methods — In vivo determination of the sun protection factor (SPF)
Kochevar, I. E. (1992). Acute Effects of Ultraviolet Radiation on Skin. In M. F. Holick & A. M. Kligman (Eds.), Biologic Effects of Light (pp. 3–10). De Gruyter.
Kohli, I., Shafi, R., Isedeh, P., Griffith, J. L., Al-Jamal, M. S., Silpa-Archa, N., Jackson, B., Athar, M., Kollias, N., Elmets, C. A., Lim, H. W., & Hamzavi, I. H. (2017). The impact of oral Polypodium leucotomos extract on ultraviolet B response: A human clinical study. Journal of the American Academy of Dermatology, 77(1), 33–41.e1.
Matsumura, Y., & Ananthaswamy, H. N. (2004). Toxic effects of ultraviolet radiation on the skin. Toxicology and Applied Pharmacology, 195(3), 298–308.
Miller, S. A., Coelho, S. G., Yamaguchi, Y., Hearing, V. J., Beer, J. Z., & de Gruijl, F. (2017). The Evaluation of Noninvasive Measurements of Erythema as a Potential Surrogate for DNA Damage in Repetitively UV-exposed Human Skin. Photochemistry and Photobiology, 93(5), 1282–1288.
Moehrle, M., Koehle, W., Dietz, K., & Lischka, G. (2000). Reduction of minimal erythema dose by sweating: Reduction of MED by sweating. Photodermatology, Photoimmunology & Photomedicine, 16(6), 260–262.
Rhodes, L. E., Gledhill, K., Masoodi, M., Haylett, A. K., Brownrigg, M., Thody, A. J., Tobin, D. J., & Nicolaou, A. (2009). The sunburn response in human skin is characterized by sequential eicosanoid profiles that may mediate its early and late phases. The FASEB Journal, 23(11), 3947–3956.
Richey, J. A., Sullivan-Toole, H., Strege, M., Carlton, C., McDaniel, D., Komelski, M., Epperley, A., Zhu, H., & Allen, I. C. (2019). Precision Implementation of Minimal Erythema Dose (MED) Testing to Assess Individual Variation in Human Inflammatory Response. Journal of Visualized Experiments, 8.
Samorano, L. P., & Reis, V. M. S. (2017). Photoprotection: Concept, Classification, and Mechanism of Action. In M. C. A. Issa & B. Tamura (Eds.), Daily Routine in Cosmetic Dermatology (Vol. 1, pp. 103–111). Springer International Publishing.
Seite, S., Medaisko, C., Christiaens, F., Bredoux, C., Compan, D., Zucchi, H., Lombard, D., & Fourtanier, A. (2006). Biological effects of simulated ultraviolet daylight: A new approach to investigate daily photoprotection. Photodermatology, Photoimmunology and Photomedicine, 22(2), 67–77.
United Nations ‐ Department of Economic and Social Affairs Population Division. World population prospects, the 2015 revision.
Waterston, K., Naysmith, L., & Rees, J. L. (2004). Physiological Variation in the Erythemal Response to Ultraviolet Radiation and Photoadaptation. Journal of Investigative Dermatology, 123(5), 958–964.
Welti, M., Ramelyte, E., Dummer, R., & Imhof, L. (2020). Evaluation of the minimal erythema dose for UVB and UVA in context of skin phototype and nature of photodermatosis. Photodermatology, Photoimmunology & Photomedicine, 36(3), 200–207.
Wu, S., Cho, E., Li, W. Q., Weinstock, M. A., Han, J., & Qureshi, A. A. (2016). History of Severe Sunburn and Risk of Skin Cancer Among Women and Men in 2 Prospective Cohort Studies. American journal of epidemiology, 183(9), 824–833.
Young, A. R. (2006). Acute effects of UVR on human eyes and skin. Progress in Biophysics and Molecular Biology, 92(1), 80–85.