Building a melanocortin house
CLINUVEL’s aim is to take our success to date and use the skills, knowledge, and technology that we have developed to bring additional melanocortin products to the patients who need them the most.
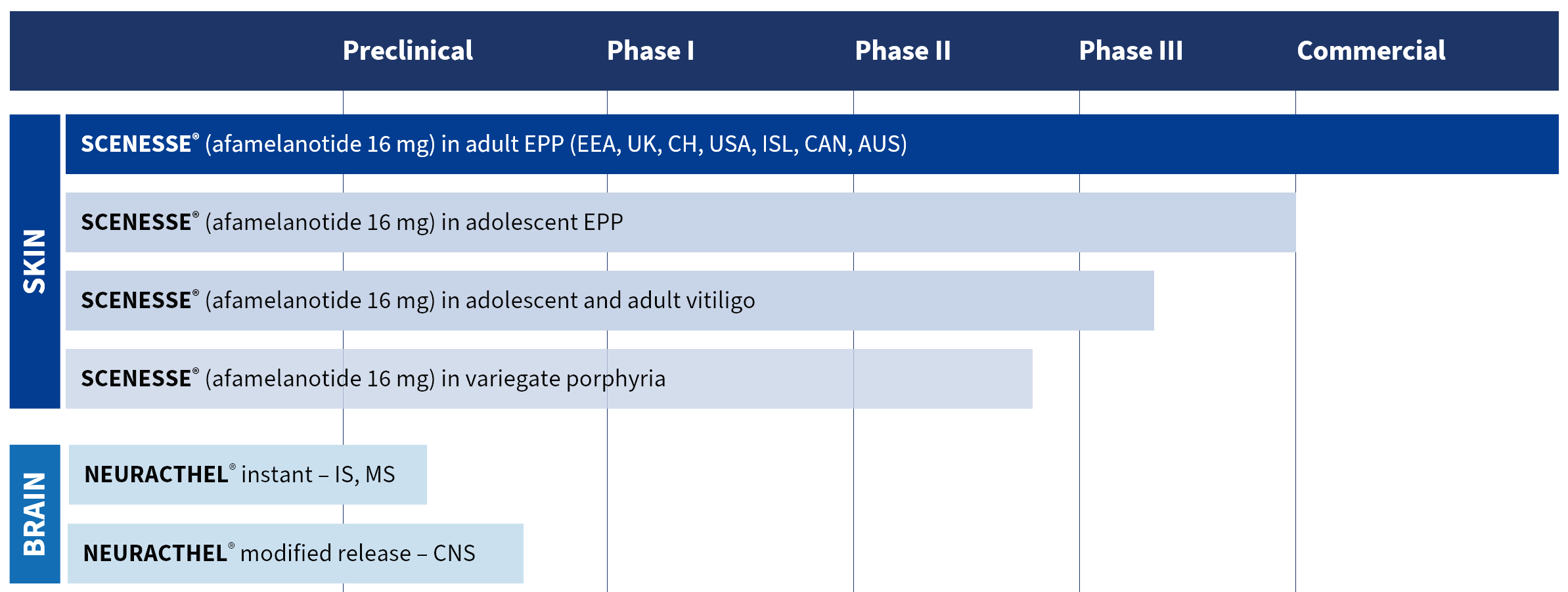
CLINUVEL has established multiple formulations of its lead melanocortin, afamelanotide, to meet the needs of patients with a range of disorders.
Alongside this work, we are also using our expertise to develop adrenocorticotropic hormone (ACTH) to diversify our portfolio of products and bring much needed treatment to patient populations who are currently underserved.
Pipeline
PRÉNUMBRA®
PRÉNUMBRA® is a liquid (non-solid) injectable formulation of afamelanotide designed for administration by a healthcare professional and intended to provide a flexible dose of afamelanotide, a synthetic analogue of natural α-melanocyte stimulating hormone.
The development of PRÉNUMBRA® will evaluate the safety and efficacy of afamelanotide in acute and systemic diseases, including stroke, as a vasoactive drug to counteract fluid formation in tissues.
PRÉNUMBRA® Instant presentation is manufactured according to current Good Manufacturing Practice (cGMP) guidelines for use in clinical trials. Further clinical targets for PRÉNUMBRA® Instant are under evaluation, including other disorders of the central nervous system (CNS).
NEURACTHEL®
CLINUVEL has a commercial agreement with one of its strategic partners for the scaled supply of adrenocorticotropic hormone (ACTH) drug substance to current Good Manufacturing Practices (cGMP) standard.
Translating its expertise in melanocortins and formulation development, CLINUVEL will be commercialising NEURACTHEL® (ACTH) in multiple dosage forms for patients in need of medical treatment.
CUV9900
CUV9900 is an α-MSH analogue being investigated by CLINUVEL as a skin protectant. CLINUVEL intends to launch CUV9900 in various new formulations. Formulation work has commenced and CLINUVEL expects the first formulations to be available for clinical testing after the commercialisation of SCENESSE® in Europe.